Chapter 5: The Endocrine System

Chapter 5: The Endocrine System
SCIENCE MASTERY ASSESSMENT
Every pre-med knows this feeling: there is so much content I have to know for the MCAT! How do I know what to do first or what's important?
While the high-yield badges throughout this book will help you identify the most important topics, this Science Mastery Assessment is another tool in your MCAT prep arsenal. This quiz (which can also be taken in your online resources) and the guidance below will help ensure that you are spending the appropriate amount of time on this chapter based on your personal strengths and weaknesses. Don't worry though— skipping something now does not mean you'll never study it. Later on in your prep, as you complete full-length tests, you'll uncover specific pieces of content that you need to review and can come back to these chapters as appropriate.
How to Use This Assessment
If you answer 0–7 questions correctly:
Spend about 1 hour to read this chapter in full and take limited notes throughout. Follow up by reviewing all quiz questions to ensure that you now understand how to solve each one.
If you answer 8–11 questions correctly:
Spend 20–40 minutes reviewing the quiz questions. Beginning with the questions you missed, read and take notes on the corresponding subchapters. For questions you answered correctly, ensure your thinking matches that of the explanation and you understand why each choice was correct or incorrect.
If you answer 12–15 questions correctly:
Spend less than 20 minutes reviewing all questions from the quiz. If you missed any, then include a quick read-through of the corresponding subchapters, or even just the relevant content within a subchapter, as part of your question review. For questions you answered correctly, ensure your thinking matches that of the explanation and review the Concept Summary at the end of the chapter.
- Which of the following associations between a hormone and its category is INCORRECT?
- Aldosterone—mineralocorticoid
- Testosterone—cortical sex hormone
- ADH—mineralocorticoid
- Cortisone—glucocorticoid
- Which of the following hormones directly stimulates a target tissue that is NOT an endocrine organ?
- ACTH
- TSH
- LH
- GH
- Increased synthetic activity of the parathyroid glands would lead to:
- an increase in renal calcium reabsorption.
- a decrease in the rate of bone resorption.
- a decrease in basal metabolic rate.
- a decrease in blood glucose concentration.
- Which of the following best describes the structure and mechanism of action of a peptide hormone?
- Cholesterol derivative that binds to a receptor on the cell surface
- Chain of amino acids that signals through a second messenger
- Chain of amino acids that directly binds to DNA to alter gene expression
- Cholesterol derivative that binds to an intracellular receptor and alters gene expression
- Iodine deficiency may result in:
- galactorrhea.
- cretinism.
- gigantism.
- hyperthyroidism.
- A patient has a very high TSH level. Which of the following would NOT cause a high TSH level?
- Autoimmune destruction of thyroid cells that produce T3 and T4
- A tumor in the hypothalamus that secretes high levels of TRH
- High levels of T4 from thyroid replacement medications
- Cancerous growth of parafollicular cells in the thyroid, destroying other cell types in the organ
- Testing of a novel hormone indicates nuclear localization and a composition of carbon, hydrogen, and oxygen. Based on these findings, how would this hormone most likely be classified?
- Peptide hormone
- Steroid hormone
- Amino acid derivative
- Direct hormone
- Which of the following is true regarding pancreatic somatostatin?
- Its secretion is increased by low blood glucose.
- It is always inhibitory.
- It is regulated by cortisol levels.
- It stimulates insulin and glucagon secretion.
- Destruction of all β-cells in the pancreas would cause:
- glucagon secretion to stop and an increase in blood glucose concentration.
- glucagon secretion to stop and a decrease in blood glucose concentration.
- insulin secretion to stop and an increase in blood glucose concentration.
- insulin secretion to stop and a decrease in blood glucose concentration.
- Which of the following is FALSE regarding aldosterone regulation?
- Renin converts the plasma protein angiotensinogen to angiotensin I.
- Angiotensin II stimulates the adrenal cortex to secrete aldosterone.
- Angiotensin I is converted to angiotensin II by angiotensin-converting enzyme.
- A decrease in blood oxygen concentrations stimulates renin production.
- A scientist discovers a new hormone that is relatively large in size and triggers the conversion of ATP to cAMP. Which of the following best describes the type of hormone that was discovered?
- Amino acid–derivative hormone
- Peptide hormone
- Steroid hormone
- Tropic hormone
- A patient presents with muscle weakness, slow movement, and calcium deposits in some tissues. A blood test reveals very low calcium levels in the blood. Administration of which of the following would be an appropriate treatment for the blood test findings?
- Calcitonin
- Parathyroid hormone
- Aldosterone
- Thymosin
- Oxytocin and antidiuretic hormone are:
- peptide hormones produced and released by the pituitary.
- steroid hormones produced and released by the pituitary.
- peptide hormones produced by the hypothalamus and released by the pituitary.
- steroid hormones produced by the hypothalamus and released by the pituitary.
- Excessive levels of dopamine in the brain are associated with psychosis. Accordingly, many antipsychotic medications block dopamine receptors. Which of the following effects may be seen in an individual taking antipsychotics?
- Increased secretion of growth hormone
- Decreased secretion of growth hormone
- Increased secretion of prolactin
- Decreased secretion of prolactin
- A genotypically female infant is born with ambiguous genitalia. Soon after birth, the infant suffers from hyponatremia, or low blood concentrations of sodium. Which endocrine organ is most likely to be affected?
- Hypothalamus
- Pituitary
- Kidneys
- Adrenal cortex
Answer Key
- C
- D
- A
- B
- B
- C
- B
- B
- C
- D
- B
- B
- C
- C
- D
Chapter 5: The Endocrine System
CHAPTER 5
THE ENDOCRINE SYSTEM
In This Chapter
5.1 Mechanisms of Hormone Action
Classification of Hormones by Chemical Structure
Classification of Hormones by Target Tissue
5.2 Endocrine Organs and Hormones
Hypothalamus
Anterior Pituitary
Posterior Pituitary
Thyroid
Parathyroid Glands
Adrenal Cortex
Adrenal Medulla
Pancreas
Gonads
Pineal Gland
Other Organs
Concept Summary
CHAPTER PROFILE
The content in this chapter should be relevant to about 9% of all questions about biology on the MCAT.
This chapter covers material from the following AAMC content categories:
3A: Structure and functions of the nervous and endocrine systems and ways in which these systems coordinate the organ systems
3B: Structure and integrative functions of the main organ systems
Introduction
The human body consists of many trillions of cells that must work together to sustain life. In order to work effectively, fuel resources must be conserved or used appropriately, such as when responding to stressful situations. In addition, organs must be able to communicate with the brain to cause changes in behavior and physiology to maintain homeostasis. As the messengers in the endocrine system, hormones play an essential role in this communication. For example, the pancreas produces insulin and glucagon. Insulin induces the transport of glucose into organs and the storage of excess glucose when blood glucose concentrations are high. Conversely, glucagon triggers the release of sugar stores which raises blood glucose concentration. Working together, these hormones ensure that there are adequate levels of glucose for organ function, but that glucose levels are not so high as to cause damage to organ systems.
Diabetes mellitus is one of the most common diseases in the United States and a major cause of morbidity and mortality. Type 1 diabetes mellitus is an autoimmune disease in which insulin-producing cells in the islets of Langerhans are destroyed. Type 2 diabetes mellitus is caused by end-organ insensitivity to insulin. In both cases, blood glucose concentrations rise to dangerous levels (sometimes up to ten times the normal concentration), which can cause significant damage to organs, including the retina of the eye, the glomeruli of the kidneys, the coronary vessels of the heart and cerebral vessels of the brain, and peripheral nerves. Left untreated (or, to be frank, even if treated in many cases), diabetes can lead to blindness, kidney failure, heart attacks, strokes, and limb amputations. Regardless of the field you enter, you will spend a significant amount of time working with diabetic patients and will have to think about the effects of this disease on other conditions and their treatment.
In this chapter, we will explore the different types of hormones and how they work. We’ll survey the various endocrine organs and discuss the hormones each one produces. This is an extremely high-yield chapter: the MCAT frequently tests not only the makeup of the endocrine system (hormones and their functions), but also the processes of the endocrine system (feedback loops and their regulation). Return to this chapter frequently; a thorough knowledge of this system will definitely pay off on Test Day.
5.1 Mechanisms of Hormone Action
LEARNING OBJECTIVES
After Chapter 5.1, you will be able to:
- Compare and contrast the traits and actions of peptide vs. steroid hormones
- Recall the process for synthesizing amino acid–derivative hormones
- Distinguish between direct and tropic hormones
The endocrine system consists of organs, known as glands, that secrete hormones. Hormones are signaling molecules that are secreted directly into the bloodstream to distant target tissues. At target tissues, hormones bind to receptors, inducing a change in gene expression or cellular functioning. Not all hormones share the same structure and function. In order to understand how each hormone functions, it is first important to understand basic hormone structure.
Classification of Hormones by Chemical Structure
Hormones can be subdivided into categories based on different criteria. First, hormones can be classified by their chemical identities. Hormones can be peptides, steroids, or amino acid derivatives.
Peptide Hormones
Peptide hormones are made up of amino acids, ranging in size from quite small (such as anti-diuretic hormone, ADH) to relatively large (such as insulin). Peptide hormones are all derived from larger precursor polypeptides that are cleaved during posttranslational modification. These smaller units are transported to the Golgi apparatus for further modifications that activate the hormones and direct them to the correct locations in the cell. Such hormones are released by exocytosis after being packaged into vesicles.
Because peptide hormones are charged and cannot pass through the plasma membrane, they must bind to an extracellular receptor. The peptide hormone is considered the first messenger; it binds to the receptor and triggers the transmission of a second signal, known as the second messenger. There are many different receptor subtypes, and the type of receptor determines what happens once the hormone has stimulated the receptor.
The connection between the hormone at the surface and the effect brought about by second messengers within the cell is known as a signaling cascade. At each step, there is the possibility of amplification. For example, one hormone molecule may bind to multiple receptors before it is degraded. Also, each receptor may activate multiple enzymes, each of which will trigger the production of large quantities of second messengers. Thus, each step can result in an increase in signal intensity. Some common second messengers are cyclic adenosine monophosphate (cAMP),inositol triphosphate (IP3), and calcium. The activation of a G protein–coupled receptor is shown in Figure 5.1. In this system, the binding of a peptide hormone triggers the receptor to either activate or inhibit an enzyme called **adenylate cyclase**, raising or lowering the levels of cAMP accordingly. cAMP can bind to intracellular targets, such as protein kinase A, which phosphorylates transcription factors like cAMP response element-binding protein (CREB) to exert the hormone’s ultimate effect. Keep in mind that protein kinase A can modify other enzymes as well as transcription factors, and therefore it can have a rapid or slow effect on the cell.
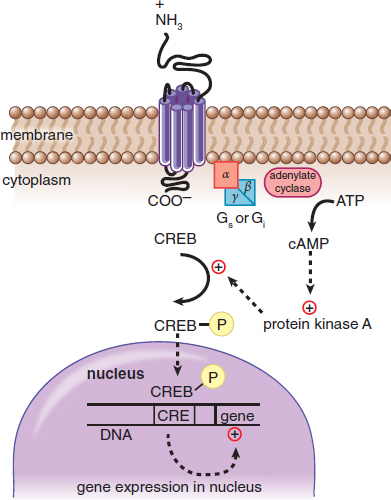
Figure 5.1. Mechanism of Action of a Peptide Hormone Peptide hormones bind to membrane-bound receptors to intiate a signal cascade, using second messengers like cAMP.
The effects of peptide hormones are usually rapid but short lived because these hormones act through second messenger cascades, which are transient. It is quicker to turn them on and off, compared with steroid hormones, but their effects do not last without relatively constant stimulation.
Because peptides are generally water-soluble, peptide hormones can travel freely in the bloodstream and usually do not require carriers. This is in stark contrast to steroid hormones, which are lipid-soluble.
KEY CONCEPT
Peptide hormones have surface receptors and act via second messenger systems. Steroid hormones bind to intracellular receptors and function by binding to DNA to alter gene transcription.
Steroid Hormones
Steroid hormones are derived from cholesterol and are produced primarily by the gonads and adrenal cortex. Because steroid hormones are derived from nonpolar molecules, they can easily cross the cell membrane. Hence, their receptors are usually intracellular (in the cytosol) or intranuclear (in the nucleus). Upon binding to the receptor, steroid hormone–receptor complexes undergo conformational changes. The receptor can then bind directly to DNA, resulting in either increased or decreased transcription of particular genes, depending on the identity of the hormone, as shown in Figure 5.2. One common form of conformational change is dimerization, or pairing of two receptor–hormone complexes. The effects of steroid hormones are slower but longer lived than peptide hormones because steroid hormones participate in gene regulation, causing alterations in the amount of mRNA and protein present in a cell by direct action on DNA.
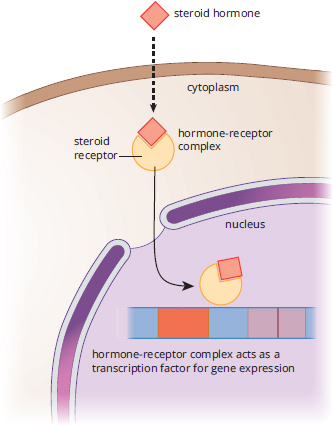
Figure 5.2. Mechanism of Action of a Steroid Hormone Estrogen, like all steroid hormones, influences cell behavior by modifying transcription.
MNEMONIC
Insulin is a peptide hormone, and it has to be released at every meal in order to be active. Thus, it has fast onset but is short-acting (like most peptide hormones). Estrogen and testosterone are steroid hormones that promote sexual maturation. This is a slower, but longer-lasting change (as is true for most steroid hormones).
Steroid hormones are not water-soluble, so they must be carried by proteins in the bloodstream to travel around the body. Some of these proteins are very specific and carry only one hormone (such as sex hormone-binding globulin), while other proteins are nonspecific (such as albumin). Note that hormones are generally inactive while attached to a carrier protein and must dissociate from the carrier to function. Therefore, levels of carrier proteins can change the levels of active hormone. For example, some conditions increase the quantity of a protein that carries thyroid hormones, thyroxine-binding globulin (TBG). This causes the body to perceive a lower level of thyroid hormone because the increased quantity of TBG binds a larger proportion of the hormone, meaning there is less free hormone available.
REAL WORLD
During pregnancy, high levels of estrogen and progesterone cause increased production of TBG, thyroxine-binding globulin. In order to compensate, people who are pregnant secrete much higher levels of the thyroid hormones. Thus, in order to diagnose thyroid disease during pregnancy, different reference values must be used.
Amino Acid–Derivative Hormones
Finally, amino acid–derivative hormones are less common than peptide and steroid hormones, but include some of the most important hormones discussed in this chapter, including epinephrine, norepinephrine, triiodothyronine, and thyroxine. These hormones are derived from one or two amino acids, usually with a few additional modifications. For example, thyroid hormones are made from tyrosine modified by the addition of several iodine atoms.
The chemistry of this family of hormones is considerably less predictable and is one of the few instances where overt memorization may be the best strategy. For instance, the catecholamines (epinephrine and norepinephrine) bind to G protein–coupled receptors, while thyroid hormones bind intracellularly.
MCAT EXPERTISE
The mechanism of action of the amino acid–derivative hormones should be memorized because it is so unpredictable. Epinephrine and norepinephrine have extremely fast onset but are short-lived, like peptide hormones—think of an adrenaline rush. Thyroxine and triiodothyronine, on the other hand, have slower onset but a longer duration, like steroid hormones—they regulate metabolic rate over a long period of time.
Classification of Hormones by Target Tissue
Some hormones, known as direct hormones, are secreted and then act directly on a target tissue. For example, insulin released by the pancreas causes increased uptake of glucose by muscles. Other hormones, known as tropic hormones, require an intermediary to act. For example, as discussed in Chapter 2 of MCAT Biology Review, gonadotropin-releasing hormone (GnRH) from the hypothalamus stimulates the release of luteinizing hormone (LH) and follicle-stimulating hormone (FSH). LH then acts on the gonads to stimulate testosterone production in males and estrogen production in females. GnRH and LH do not cause direct changes in the physiology of muscle, bone, and hair follicles; rather, they stimulate the production of another hormone by another endocrine gland that acts on these target tissues. Tropic hormones usually originate in the brain and anterior pituitary gland, allowing for the coordination of multiple processes within the body.
MNEMONIC
Most peptide and amino acid–derivative hormones have names that end in –in or –ine (insulin, vasopressin, thyroxine, triiodothyronine, and so on). Most steroid hormones have names that end in –one, –ol, or –oid (testosterone, aldosterone and other mineralocorticoids, cortisol and other glucocorticoids, and so on). This is not exhaustive, but may help you identify the chemistry of a hormone on Test Day.
MCAT CONCEPT CHECK 5.1
Before you move on, assess your understanding of the material with these questions.
- Compare and contrast peptide and steroid hormones based on the following criteria:
Criterion Peptide Hormones Steroid Hormones
Chemical precursor Location of receptor Mechanism of action Method of travel in the bloodstream Speed of onset Duration of action
- How are amino acid–derivative hormones synthesized?
- What is the difference between a direct and a tropic hormone?
- Direct hormone:
- Tropic hormone:
5.2 Endocrine Organs and Hormones
LEARNING OBJECTIVES
After Chapter 5.2, you will be able to:
- Recall the hormones involved in calcium homeostasis and their impact on blood calcium
- Identify the tissue that synthesizes catecholamines and the major catecholamines it produces
- List the pancreatic hormones, their regulators, and their impact on blood glucose concentration
- Recall details about the hormones involved in water homeostasis, including their production, action, and ultimate impact on blood volume and osmolarity
- Recall the releasing hormones produced by the hypothalamus, their pituitary targets, and the end result of each signaling pathway on the final target organ:
The hypothalamus, the pituitary, the thyroid, the parathyroid glands, the adrenal glands, the pancreas, the gonads (testes and ovaries), and the pineal gland are all endocrine glands, as shown in Figure 5.3. Each of these organs is capable of synthesizing and secreting one or more hormones. Furthermore, there are collections of cells within organs, such as the kidneys, gastrointestinal glands, heart, and thymus, that serve important endocrine roles. The organs in this second group are traditionally not called endocrine organs because hormone production is not their main function.
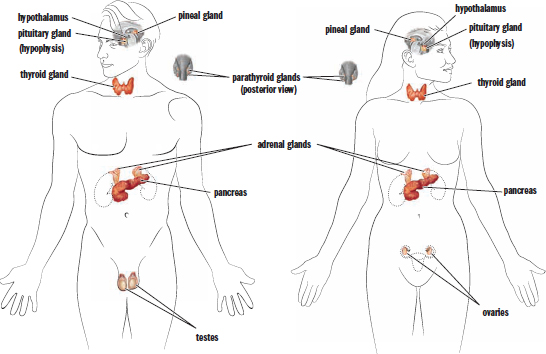
Figure 5.3. Organs of the Endocrine System Endocrine organs produce hormones that are secreted into the bloodstream to act on distant target tissues.
Now that we have discussed the mechanisms through which hormones act and their classification, we can discuss the individual endocrine organs and the hormones secreted by each.
Hypothalamus
Let’s begin with the hypothalamus, the bridge between the nervous and endocrine systems. By regulating the pituitary gland through tropic hormones, the hypothalamus is capable of having organism-wide effects. The hypothalamus is located in the forebrain, directly above the pituitary gland and below the thalamus (hence the name hypothalamus). Because the hypothalamus and the pituitary are close to each other, the hypothalamus controls the pituitary through paracrine release of hormones into a portal system that directly connects the two organs. The hypothalamus receives input from a wide variety of sources. For example, a part of the hypothalamus called the *suprachiasmatic** nucleus* receives some of the light input from the retinae and helps to control sleep–wake cycles. Other parts of the hypothalamus respond to increases in blood osmolarity. Still other parts of the hypothalamus regulate appetite and satiety.
BRIDGE
The hypothalamus contains a number of nuclei in its three sections, called the lateral, ventromedial, and anterior hypothalamus. These nuclei play roles in emotional experience, aggressive behavior, sexual behavior, metabolism, temperature regulation, and water balance. The parts of the hypothalamus are discussed in Chapter 1 of MCAT Behavioral Sciences Review.
The release of hormones by the hypothalamus is regulated by negative feedback. Negative feedback occurs when a hormone (or product) later in the pathway inhibits hormones (or enzymes) earlier in the pathway. This type of feedback maintains homeostasis and conserves energy by restricting production of substances that are already present in sufficient quantities. The hypothalamus and pituitary gland are inextricably linked. The pituitary gland has an anterior and posterior component, each with a unique interaction with the hypothalamus. We will discuss each in turn.
Interactions with the Anterior Pituitary
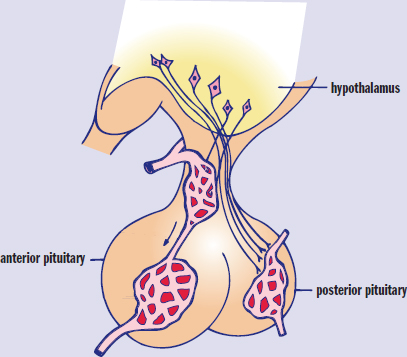
The hypothalamus secretes compounds into the hypophyseal portal system, which is a blood vessel system that directly connects the hypothalamus with the anterior pituitary, as shown in Figure 5.4. Thus, hormones released from the hypothalamus travel directly to the anterior pituitary and cannot be found in appreciable concentrations in the systemic circulation. Note that hypophysis is an alternative term for the pituitary. Once hormones have been released from the hypothalamus into this portal bloodstream, they travel down the pituitary stalk and bind to receptors in the anterior pituitary, stimulating the release of other hormones.
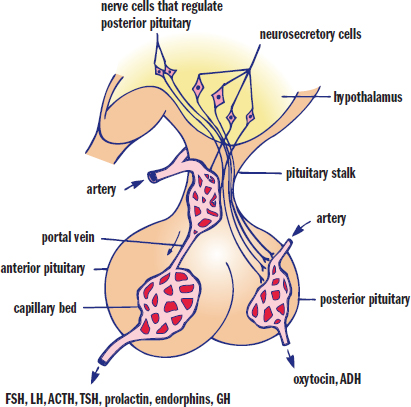
Figure 5.4. The Hypophyseal Portal System A system of blood vessels connects the hypothalamus to the pituitary.
The hypothalamus secretes several different tropic hormones. The following indicates each hormone released by the hypothalamus and the hormone(s) released by the anterior pituitary in response:
- Gonadotropin-releasing hormone (GnRH) → follicle-stimulating hormone (FSH) and luteinizing hormone (LH)
- Growth hormone–releasing hormone (GHRH) → growth hormone (GH)
- Thyroid-releasing hormone (TRH) → thyroid-stimulating hormone (TSH)
- Corticotropin-releasing factor (CRF) → adrenocorticotropic hormone (ACTH)
KEY CONCEPT
Although it seems as if the anterior pituitary has all the power in the endocrine system, it is controlled by the hypothalamus, which is located directly above it.
There is one exception to this pattern—prolactin-inhibiting factor (PIF), which is actually dopamine, is released by the hypothalamus and causes a decrease in prolactin secretion.
KEY CONCEPT
Whereas most of the hormones in the anterior pituitary require a factor from the hypothalamus to be released, prolactin is the exception. As long as the hypothalamus releases PIF (which is actually dopamine), no prolactin will be released. It is the absence of PIF that allows prolactin to be released.
Each of the tropic hormones then causes the release of another hormone from an endocrine gland that has negative feedback effects. For example, release of CRF from the hypothalamus will stimulate the anterior pituitary to secrete ACTH. ACTH will then cause the adrenal cortex to increase the level of cortisol being secreted into the blood. However, cortisol is detrimental when levels become too high. To prevent excess cortisol secretion, cortisol inhibits the hypothalamus and anterior pituitary from releasing CRF and ACTH, respectively, as shown in Figure 5.5. This makes sense because CRF and ACTH have already accomplished their desired effect: getting more cortisol into the blood. What does this mean in terms of receptors in the hypothalamus and pituitary? Cortisol receptors must be present in these organs; otherwise, they wouldn’t be able to recognize that cortisol levels had increased. Three-organ systems like these are commonly referred to as axes; for example, the hypothalamic–pituitary–adrenal (HPA) axis, the hypothalamic–pituitary–ovarian (HPO) axis, and so on.
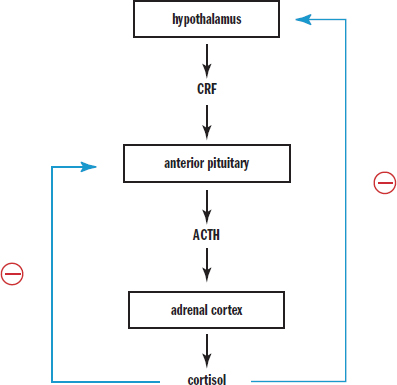
Figure 5.5. Hypothalamic Negative Feedback Mechanism
Interactions with the Posterior Pituitary
The posterior pituitary does not receive tropic hormones through the hypophyseal portal system. Rather, neurons in the hypothalamus send their axons down the pituitary stalk directly into the posterior pituitary, which can then release oxytocin and antidiuretic hormone. Oxytocin stimulates uterine contractions during labor, as well as milk letdown during lactation. There is evidence that oxytocin is also involved in bonding behavior. Antidiuretic hormone (ADH, also called vasopressin) increases reabsorption of water in the collecting ducts of the kidneys. ADH is secreted in response to increased plasma osmolarity, or increased concentration of solutes within the blood.
REAL WORLD
A tumor of the pituitary gland may result in compression of the portal system that connects the pituitary to the hypothalamus. This will block the ability of PIF to reach the pituitary and exert its effect. Thus, more prolactin will be released. This may result in lactation (galactorrhea), even in males. Thus, milk production in a male or nonpregnant female should lead a physician to suspect the presence of a pituitary tumor.
Anterior Pituitary
As described earlier, the pituitary gland is divided into anterior and posterior sections. Because this distinction has already been covered, our discussion of the pituitary gland here will focus on the hormones released by each section.
The anterior pituitary synthesizes and secretes seven different products. Four of these are tropic hormones, while the other three are direct hormones.
MNEMONIC
Products of the anterior pituitary:
FLAT PEG
- Follicle-stimulating hormone (FSH)
- Luteinizing hormone (LH)
- Adrenocorticotropic hormone (ACTH)
- Thyroid-stimulating hormone (TSH)
- Prolactin
- Endorphins
- Growth hormone (GH)
Additionally, the four hormones inFLAT are all tropic hormones, while the three hormones in PEG are all direct hormones.
Tropic Hormones
We are going to mention the tropic hormones only briefly here. These hormones work by causing the release of another hormone at the organ level. Thus, we will discuss the tropic hormones in tandem with the endocrine organ on which they act. The release of both follicle-stimulating hormone (FSH) and luteinizing hormone (LH) is stimulated by gonadotropin-releasing hormone (GnRH) from the hypothalamus. These two hormones act on the gonads (testes and ovaries). The release of adrenocorticotropic hormone (ACTH) is stimulated by corticotropin-releasing factor (CRF) from the hypothalamus; ACTH acts on the adrenal cortex. The release of thyroid-stimulating hormone (TSH) is stimulated by thyroid-releasing hormone (TRH) from the hypothalamus; TSH acts on the thyroid.
Direct Hormones
Prolactin is more important in females than in males; it stimulates milk production in the mammary glands. Milk production in the male is always pathologic. During pregnancy, estrogen and progesterone levels are high. In addition, prolactin, a hormone that increases milk production, is also secreted by the anterior pituitary. Prolactin is an unusual hormone in that the release of dopamine from the hypothalamus decreases its secretion. The high levels of estrogen and progesterone allow for the development of milk ducts in preparation for lactation, but it is not until shortly after the expulsion of the placenta, when estrogen, progesterone, and dopamine levels drop, that the block on milk production is removed and lactation actually begins.
Milk ejection occurs when the newborn infant latches on to the breast. Nipple stimulation causes activation of the hypothalamus, resulting in two different reactions. First, oxytocin is released from the posterior pituitary, resulting in contraction of the smooth muscle of the breast and ejection of milk through the nipple. Second, the hypothalamus stops releasing dopamine onto the anterior pituitary, which allows prolactin release, causing production of milk and regulation of the milk supply.
Endorphins decrease the perception of pain. For example, after completing a marathon, many people will say they are on an endorphin “high” or “rush.” Endorphins mask the pain from having run 26.2 miles and can even induce a sense of euphoria. Many pharmaceutical agents, such as morphine, mimic the effect of these naturally occurring painkillers.
Growth hormone (GH) is named for exactly what it does: it promotes the growth of bone and muscle. This sort of growth is energetically expensive and requires large quantities of glucose. Growth hormone prevents glucose uptake in certain tissues (those that are not growing) and stimulates the breakdown of fatty acids. This increases the availability of glucose overall, allowing muscle and bone to use it. GH release is stimulated by growth hormone–releasing hormone (GHRH) from the hypothalamus.
Bone growth originates in special regions of the bone known as epiphyseal plates, which seal shut during puberty. An excess of GH released in childhood (before this closure) can cause gigantism, and a deficit results in dwarfism. In adults, the situation is slightly different. Because the long bones are sealed, GH still has an effect, but it is primarily in the smaller bones. The resulting medical condition is known as acromegaly. The bones most commonly affected are those in the hands, feet, and head. Patients with acromegaly tend to seek medical help because they have had to buy larger shoes, cannot wear their rings, and can no longer fit into their hats.
Posterior Pituitary
The posterior pituitary contains the nerve terminals of neurons with cell bodies in the hypothalamus. As mentioned earlier, the posterior pituitary receives and stores two hormones produced by the hypothalamus: ADH and oxytocin.
ADH is secreted in response to low blood volume (as sensed by baroreceptors) or increased blood osmolarity (as sensed by osmoreceptors), shown in Figure 5.6. Its action is at the level of the collecting duct, where it increases the permeability of the duct to water. This increases the reabsorption of water from the filtrate in the nephron. This results in greater retention of water, which results in increased blood volume and higher blood pressure.
KEY CONCEPT
The two hormones released from the posterior pituitary are actually synthesized in the hypothalamus and simply released from the posterior pituitary gland. The posterior pituitary does not synthesize any hormones itself.
Oxytocin is secreted during childbirth and allows for coordinated contraction of uterine smooth muscle. Its secretion may also be stimulated by suckling, as it promotes milk ejection through contraction of smooth muscle in the breast. Finally, oxytocin may be involved in bonding behavior. Oxytocin is unusual in that it has a positive feedback loop: the release of oxytocin promotes uterine contraction, which promotes more oxytocin release, which promotes stronger uterine contractions, and so on. Positive feedback loops can usually be identified by a “spiraling forward” scheme and usually have a definitive endpoint—in this case, delivery.
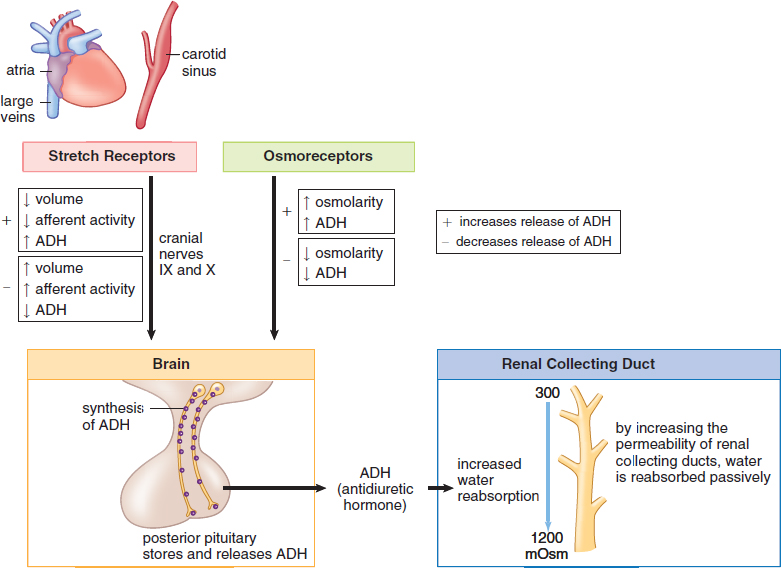
Figure 5.6. Antidiuretic Hormone (ADH)
Thyroid
The thyroid is controlled by thyroid-stimulating hormone from the anterior pituitary. The thyroid is on the front surface of the trachea; it can be palpated (felt) as an organ near the base of the neck that moves up and down with swallowing. The thyroid has two major functions: setting basal metabolic rate and promoting calcium homeostasis. It mediates the first effect by releasing triiodothyronine (T3) and thyroxine (T4), while it carries out the second effect through the release of calcitonin.
Triiodothyronine and Thyroxine
Triiodothyronine (T3) and thyroxine (T4) are both produced by the iodination of the amino acid tyrosine in the follicular cells of the thyroid. The numbers 3 and 4 refer to the number of iodine atoms attached to the tyrosine. Thyroid hormones are capable of resetting the basal metabolic rate of the body by making energy production more or less efficient, as well as altering the utilization of glucose and fatty acids. Increased amounts of T3 and T4 will lead to increased cellular respiration. This leads to increased protein and fatty acid turnover by speeding up both synthesis and degradation of these compounds. High plasma levels of thyroid hormones will lead to decreased TSH and TRH synthesis; negative feedback prevents excessive secretion of T3 and T4, as shown in Figure 5.7.
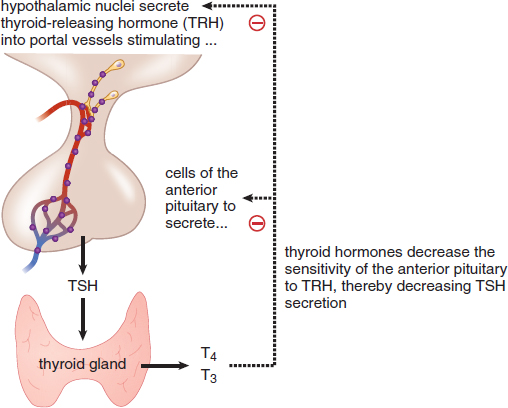
Figure 5.7. Thyroid Hormone Negative Feedback Mechanism
A deficiency of iodine or inflammation of the thyroid may result in hypothyroidism, in which thyroid hormones are secreted in insufficient amounts or not at all. The condition is characterized by lethargy, decreased body temperature, slowed respiratory and heart rate, cold intolerance, and weight gain. Thyroid hormones are required for appropriate neurological and physical development in children. Most children are tested at birth for appropriate levels because a deficiency will result in intellectual disability and developmental delay (cretinism).
An excess of thyroid hormone, which may result from a tumor or thyroid overstimulation, is called hyperthyroidism. We can predict the clinical course of this syndrome by considering the opposite of each of the effects seen in hypothyroidism: heightened activity level, increased body temperature, increased respiratory and heart rate, heat intolerance, and weight loss.
Calcitonin
If we were to examine thyroid tissue under a light microscope, we would see two distinct cell populations within the gland. Follicular cells produce thyroid hormones and C-cells (also called parafollicular cells) produce calcitonin. Calcitonin decreases plasma calcium levels in three ways: by increasing calcium excretion from the kidneys, by decreasing calcium absorption from the gut, and by increasing storage of calcium in the bone. High levels of calcium in the blood stimulate secretion of calcitonin from the C-cells.
MNEMONIC
Calcitonin tones down calcium levels in the blood.
Parathyroid Glands
The parathyroids are four small pea-sized structures that sit on the posterior surface of the thyroid. The hormone produced by the parathyroid glands is aptly named parathyroid hormone (PTH). PTH serves as an antagonistic hormone to calcitonin, raising blood calcium levels; specifically, it decreases excretion of calcium by the kidneys, increases absorption of calcium in the gut (via vitamin D), and increases bone resorption, thereby freeing up calcium, as shown in Figure 5.8. Like the hormones we have already seen, PTH is also subject to feedback inhibition. As levels of plasma calcium rise, PTH secretion is decreased. Parathyroid hormone also promotes phosphorus homeostasis by increasing the resorption of phosphate from bone and reducing reabsorption of phosphate in the kidney (thus promoting its excretion in the urine).
KEY CONCEPT
Calcium is an exceptionally important ion. The critically important functions of calcium include:
- Bone structure and strength
- Release of neurotransmitters from neurons
- Regulation of muscle contraction
- Clotting of blood (calcium is a cofactor)
In addition, calcium also plays a role in cell movement and exocytosis of cellular materials.
KEY CONCEPT
Just like glucagon and insulin, PTH and calcitonin are antagonistic to each other. We should think of these hormones as a pair with the primary function of regulating calcium levels in the blood. PTH increases serum calcium levels, whereas calcitonin decreases calcium levels.
PTH also activates vitamin D, which is required for the absorption of calcium and phosphate in the gut. The overall effect of parathyroid hormone, therefore, is a significant increase in blood calcium levels with little effect on phosphate (the absorption of phosphate in the gut and its excretion in the kidney somewhat cancel each other).
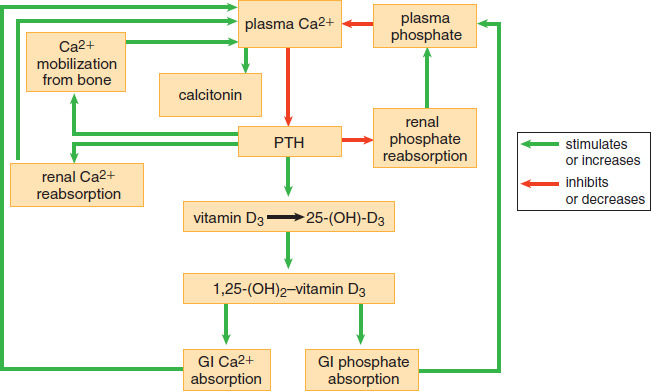
Figure 5.8. Calcium and Phosphorus Homeostasis
BIOLOGY GUIDED EXAMPLE WITH EXPERT THINKING
Patients with mutations of the THRA (thyroid hormone receptor alpha) gene exhibit classical features of hypothyroidism. Researchers created a mouse expressing a mutated TRα1 (denoted as PV; Thra1PV/+ mouse) that faithfully reproduces the classical hypothyroidism seen in patients. TRα1PV is a dominant negative mutant and cannot bind T3. Researchers then rendered Thra1PV/+ mice hypothyroidic by treating them with propylthiouracil (PTU). PTU is a medication used to treat hyperthyroidism by inhibiting the enzyme thyroperoxidase. PTU-treated mice were then treated with T3 to induce symptoms of hyperthyroidism. Results are summarized in Figure 1. These findings are consistent with earlier reports that the feedback loop in the pituitary-thyroid axis is not affected by expressing TRα1PV mutant in Thra1PV/+ mice. Topic: hypothyroidism; some outside knowledge of the endocrine system might be necessary. Specific mutation of THRA cannot bind T3 and mice with mutation have hypothyroidism PTU: medicine to treat hyperthryoidism, used to induce hypothyroidism in these mice Findings are consistent with idea that the feedback loop is not affected
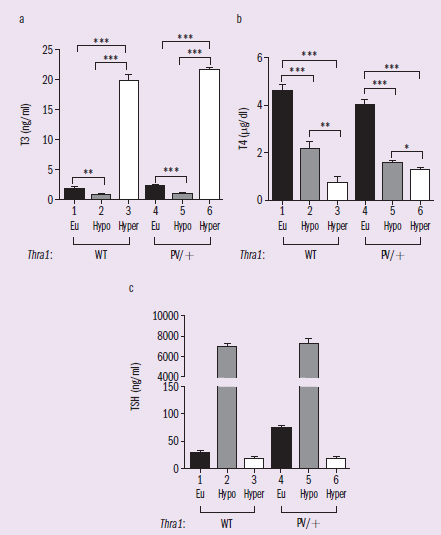
Figure 1 Thyroid experiment results. Eu = euthyroid condition.
IVs: Eu, Hypo, Hyper DVs: T3, T4, TSH Trends: Euthryoid means the thyroid is kept normal, so this is the control. The changes in T3, T4, and TSH are pretty consistent for each condition (Eu, Hypo, Hyper) between WT and PV/+ mice.
Adapted from Park, S., Han, C. R., Park, J. W., Zhao, L., Zhu, X., Willingham, M., … Cheng, S. Y. (2017). Defective erythropoiesis caused by mutations of the thyroid hormone receptor α gene. PLoS Genetics, 13(9), e1006991. doi:10.1371/journal.pgen.1006991.
Why are TSH levels elevated in mice given propylthiouracil (PTU)?
A question like this is asking us to explain the underlying biological cause for an observed phenomenon. The MCAT often tests our ability to reason with a concept or mechanism that we are already familiar with. For this question, the stated change to the system is “propylthiouracil” and the effect observed is “elevated TSH levels”. It is now our job to determine how the two are related.
First, we‘ll want to identify what information we’ll need, both from the passage and from our science background. MCAT questions will often intentionally include terms that we aren‘t familiar with. The key to answering these questions, even if we’re not familiar with the phenomenon described, is finding the relevant information from the passage and using that information in conjunction with our scientific understanding to solve the problem. We already identified the change to the system in this question as the application of PTU. According to the passage, PTU is a medication that inhibits thyroperoxidase and it is used to treat hyperthyroidism. In the experiment, they used PTU to “render[ed] Thra1PV/+ mice hypothyroidic”. If we look to Figure 1A, we can see that in the T3 and T4 graphs, the hypothyroid (gray) bar is significantly smaller than the euthyroid (black) bar. If we weren't sure what euthyroid referred to, we could infer that, given that the other two categories in each graph are hypothyroid and hyperthyroid, this must be wild-type or normal function. Based on these data and the context from the passage, it is reasonable to infer that PTU is a drug that functions by lowering the production of thyroid hormone (T3 and T4).
Now we must consider how having low thyroid hormones would be related to elevated TSH levels. TSH is a tropic hormone released from the anterior pituitary, and it is regulated by a negative feedback mechanism involving thyroid hormone. Specifically, we should know that the hypothalamus releases thyroid-releasing hormone (TRH), which causes the anterior pituitary to release thyroid-stimulating hormone (TSH). TSH acts upon the thyroid to stimulate the release of thyroid hormone triiodothyronine (T3) and thyroxine (T4). T3 and T4 then act as negative feedback on the hypothalamus and the pituitary gland, lowering TRH and TSH levels. We can reason that, if T3 and T4 levels were low, TRH and TSH would be continuously produced, as they would not be inhibited by the presence of T3 and T4.
The mice in the experiment have normally functioning endocrine glands prior to treatment. We can always assume this to be the case unless the passage explicitly states otherwise: subjects should be assumed to be healthy individuals with normal hormone levels. When PTU is administered, the thyroid hormone levels in the mice decreased. As a result, there is now less thyroid hormone in circulation. As we predicted, there is now little to no negative feedback on the hypothalamus and the anterior pituitary gland. TRH and TSH levels in the mice would be elevated as a result of this lack of feedback. Normally, that would work to create more T3 and T4, but in this case, the mice are under the influence of PTU, and despite TSH stimulation, the thyroid will not be able to produce more T3 and T4. The cycle will continue, and more TRH and TSH will be secreted.
In short, the reason why TSH level is elevated in mice administered with PTU is that there is no T3 or T4 to activate the negative feedback mechanism on TSH and TRH, which “tricks” the brain into secreting more TSH (and TRH).
Adrenal Cortex
The adrenal glands are located on top of the kidneys. Adrenal actually translates to near or next to the kidney. Each adrenal gland consists of a cortex and a medulla. This distinction is more than anatomical. Each part of the gland is responsible for the secretion of different hormones. The adrenal cortex secretes corticosteroids. These are steroid hormones that can be divided into three functional classes: glucocorticoids, mineralocorticoids, and cortical sex hormones.
Glucocorticoids
Glucocorticoids are steroid hormones that regulate glucose levels. In addition, these hormones also affect protein metabolism. The two glucocorticoids most likely to be tested on the MCAT are cortisol and cortisone. These hormones raise blood glucose by increasing gluconeogenesis and decreasing protein synthesis. Cortisol and cortisone can also decrease inflammation and immunologic responses. Cortisol is known as a stress hormone because it is released in times of physical or emotional stress. This increases blood sugar and provides a ready source of fuel in case the body must react quickly to a dangerous stimulus.
REAL WORLD
Many people who suffer from joint pain are treated with glucocorticoid injections into the joint space to decrease inflammation. In addition, glucocorticoids are used to treat systemic inflammation caused by allergic reactions or autoimmune disease.
Glucocorticoid release is under the control of adrenocorticotropic hormone (ACTH) as described earlier. Corticotropin-releasing factor (CRF) from the hypothalamus promotes release of adrenocorticotropic hormone (ACTH) from the anterior pituitary, which promotes release of glucocorticoids from the adrenal cortex.
Mineralocorticoids
Mineralocorticoids are used in salt and water homeostasis; their most profound effects are on the kidneys. The most noteworthy mineralocorticoid is aldosterone, which increases sodium reabsorption in the distal convoluted tubule and collecting duct of the nephron. Water follows the sodium cations into the bloodstream, increasing blood volume and pressure. Since water and sodium ions flow together, plasma osmolarity remains unchanged; this is in contrast to ADH, which only increases water reabsorption (decreasing plasma osmolarity). Aldosterone also decreases the reabsorption of potassium and hydrogen ions in these same segments of the nephron, promoting their excretion in the urine.
REAL WORLD
In addition to stimulating the secretion of aldosterone, which increases blood volume and hence blood pressure, angiotensin II also increases blood pressure directly through a powerful vasoconstrictive effect and increases heart rate. Angiotensin-converting enzyme (ACE) inhibitors block the conversion of angiotensin I to angiotensin II, inhibiting vasoconstriction. Therefore, ACE inhibitors are frequently prescribed for the treatment of high blood pressure and congestive heart failure. In the latter case, vasodilation helps reduce vascular resistance, decreasing the pressure against which the failing heart must pump. ACE inhibitors’ generic names end with –pril (lisinopril, enalapril, ramipril).
Unlike the glucocorticoids, aldosterone is primarily under the control of the renin–angiotensin–aldosterone system, as shown in Figure 5.9. Decreased blood pressure causes the juxtaglomerular cells of the kidney to secrete renin, which cleaves an inactive plasma protein, angiotensinogen, to its active form, angiotensin I. Angiotensin I is then converted to angiotensin II by angiotensin-converting enzyme (ACE) in the lungs. Angiotensin II stimulates the adrenal cortex to secrete aldosterone. Once blood pressure is restored, there is a decreased drive to stimulate renin release, thus serving as the negative feedback mechanism for this system.
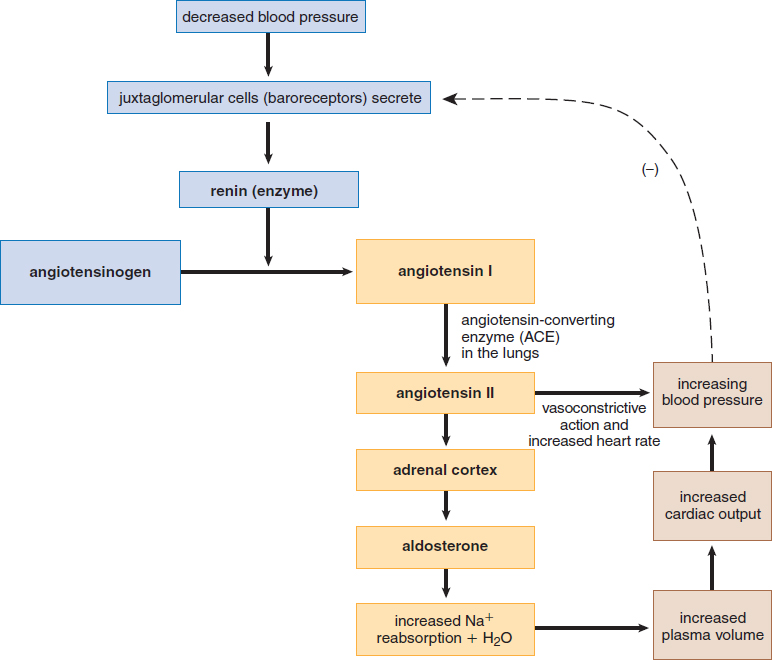
Figure 5.9. The Renin–Angiotensin–Aldosterone System
Cortical Sex Hormones
The adrenal glands also make cortical sex hormones (androgens andestrogens). Because the testes already secrete large quantities of androgens, adrenal testosterone plays a relatively small role in male physiology. But because the ovaries secrete far smaller amounts of androgens, females are much more sensitive to disorders of cortical sex hormone production. For example, certain enzyme deficiencies in the synthetic pathways of other adrenal cortex hormones result in excess androgen production in the adrenal cortex. Such a deficiency would result in no obvious phenotypic effects in a male fetus; however, a genotypic female may be born with ambiguous or masculinized genitalia due to the presence of excess cortical sex hormones. Males can be affected by similar disorders if they lead to excessive production of estrogens.
MNEMONIC
Functions of the corticosteroids:
The 3 S’s
- Salt (mineralocorticoids)
- Sugar (glucocorticoids)
- Sex (cortical sex hormones)
Adrenal Medulla
Nestled inside the adrenal cortex is the adrenal medulla. A derivative of the nervous system, this organ is responsible for the production of the sympathetic hormones epinephrine and norepinephrine. The specialized nerve cells in the medulla are capable of secreting these compounds directly into the bloodstream. Both epinephrine and norepinephrine are amino acid–derivative hormones that belong to a larger class of molecules known as catecholamines.
Much like the sympathetic component of the autonomic nervous system, the hormones released from the adrenal medulla have diverse system-wide effects, all centered on the fight-or-flight response. Epinephrine can increase the breakdown of glycogen to glucose (glycogenolysis) in both liver and muscle, as well as increase the basal metabolic rate. Both epinephrine and norepinephrine will increase heart rate, dilate the bronchi, and shunt blood flow to the systems that would be used in a sympathetic response. That is, there is vasodilation of blood vessels leading to increased bloodflow to the skeletal muscle, heart, lungs, and brain. Concurrently, vasoconstriction decreases bloodflow to the gut, kidneys, and skin. Note that the stress response involves both cortisol and epinephrine. Classically, cortisol is understood to mediate long-term (slow) stress responses, while catecholamines are understood to control short-term (fast) stress responses. In fact, cortisol actually increases the synthesis of catecholamines as well, resulting in an increase in catecholamine release.
Pancreas
The pancreas has both exocrine and endocrine functions. Exocrine tissues secrete substances directly into ducts; the pancreas produces a number of digestive enzymes, as discussed in Chapter 9 of MCAT Biology Review. From an endocrine standpoint, small clusters of hormone-producing cells are grouped together into islets of Langerhans throughout the pancreas, as shown in Figure 5.10. Islets contain three distinct types of cells: alpha (α), beta (β), and delta (δ) cells. Each cell type secretes a different hormone: α-cells secrete glucagon, β-cells secrete insulin, and δ-cells secrete somatostatin.
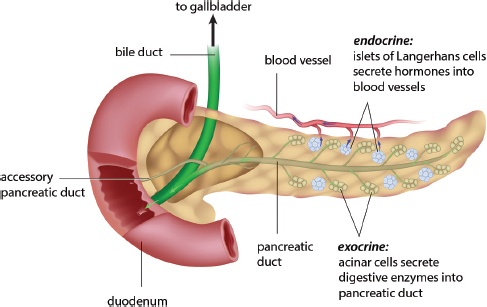
Figure 5.10. Anatomy of the Pancreas Islets of Langerhans are scattered throughout the pancreas and carry out the endocrine function of the organ.
Glucagon
Glucagon is secreted during times of fasting. When glucose levels are low, glucagon increases glucose production by triggering glycogenolysis, gluconeogenesis, and the degradation of protein and fat. In addition to low blood glucose concentrations, certain gastrointestinal hormones (such as cholecystokinin and gastrin) increase glucagon release from α-cells. When blood glucose concentrations are high, glucagon release is inhibited.
MNEMONIC
Glucagon levels are high when glucose is gone.
Insulin
Insulin is antagonistic to glucagon and is therefore secreted when blood glucose levels are high, as shown in Figure 5.11. Insulin induces muscle and liver cells to take up glucose and store it as glycogen for later use. In addition, because it is active when glucose levels are high, insulin stimulates anabolic processes such as fat and protein synthesis.
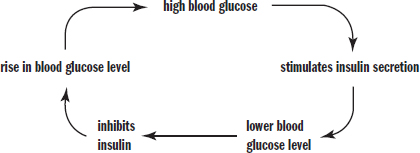
Figure 5.11. Insulin Has a Direct Relationship with Blood Glucose Concentration When blood glucose levels are high, insulin levels rise, causing cells to take up glucose from the blood; when blood glucose levels are low, insulin levels remain low as well.
In excess, insulin will cause hypoglycemia, which is characterized by low blood glucose concentration. Underproduction, insufficient secretion, or insensitivity to insulin all can result in diabetes mellitus, which is clinically characterized by hyperglycemia (excess glucose in the blood). In the kidneys, excessive glucose in the filtrate will overwhelm the nephron’s ability to reabsorb glucose, resulting in its presence in the urine. Because it is an osmotically active particle and does not readily cross the cell membrane, the presence of glucose in the filtrate leads to excess excretion of water and an increase—that is sometimes quite dramatic—in the urine volume. Therefore, patients who have diabetes often report polyuria (increased frequency of urination) and polydipsia (increased thirst). There are two types of diabetes mellitus. Type I (insulin-dependent) diabetes mellitus is caused by autoimmune destruction of the β-cells of the pancreas, resulting in low or absent insulin production. People who have type I diabetes require regular injections of insulin to prevent hyperglycemia and to permit uptake of glucose into cells. Type II (non-insulin-dependent) diabetes mellitus is the result of receptor-level resistance to the effects of insulin. Type II diabetes mellitus is partially inherited and partially due to environmental factors, such as high-carbohydrate diets and obesity. Certain pharmaceutical agents can be taken orally to help the body more effectively use the insulin it produces. These individuals require insulin only when their bodies can no longer control glucose levels, even when aided by these medications.
KEY CONCEPT
Insulin decreases plasma glucose. Glucagon increases plasma glucose. Growth hormone, glucocorticoids, and epinephrine are also capable of increasing plasma glucose. These hormones that raise blood glucose levels are commonly called counterregulatory hormones.
Somatostatin
Somatostatin is an inhibitor of both insulin and glucagon secretion. High blood glucose and amino acid concentrations stimulate its secretion. Somatostatin is also produced by the hypothalamus, where it decreases growth hormone secretion in addition to its effects on insulin and glucagon.
Gonads
Because reproductive endocrinology is discussed in detail in Chapter 2 of *MCAT Biology** Review*, we offer only a brief overview in this chapter. The testes secrete testosterone in response to stimulation by gonadotropins (LH and FSH). Testosterone causes sexual differentiation of the male during gestation and also promotes the development and maintenance of secondary sex characteristics in males, such as axillary and pubic hair, deepening of the voice, and muscle growth.
The ovaries secrete estrogen and progesterone in response to gonadotropins. Estrogen is involved in development of the female reproductive system during gestation and also promotes the development and maintenance of secondary sex characteristics in females, such as axillary and pubic hair, breast growth, and body fat redistribution. These two steroid hormones also govern the menstrual cycle as well as pregnancy.
Pineal Gland
The pineal gland is located deep within the brain, where it secretes the hormone melatonin. The precise mechanism of this hormone is unclear, although it has been demonstrated to be involved in circadian rhythms. Blood levels of melatonin are at least partially responsible for the sensation of sleepiness. The pineal gland receives projections directly from the retina, but is not involved in vision; it is hypothesized that the pineal gland responds to decreases in light intensity by releasing melatonin.
REAL WORLD
Melatonin has enjoyed somewhat of a wonder drug status over the past decade as it is touted as a remedy for everything from jet lag to aging. Certainly, one effect of melatonin is to cause profound drowsiness, hence its use in “resetting” one’s daily rhythm. Melatonin is available over the counter in health food stores, but the long-term effects of melatonin therapy are currently unknown.
Other Organs
In addition to the organs listed above, specific cells and tissues in other organs exhibit endocrine functions. In the gastrointestinal tract, endocrine tissue can be found in both the stomach and intestine. Many gastrointestinal peptides have been identified; important ones include secretin, gastrin, and cholecystokinin. The specific functions of these hormones are discussed in Chapter 9 of MCAT Biology Review, but as we might expect for the digestive system, the stimulus for release of most of these peptides is the presence of specific nutrients.
The kidneys play a role in water balance. As mentioned earlier, ADH increases water permeability in the collecting duct, and the renin–angiotensin–aldosterone system increases sodium and water reabsorption in the distal convoluted tubule and collecting duct. The kidneys also produce erythropoietin, which stimulates bone marrow to increase production of erythrocytes (red blood cells). It is secreted in response to low oxygen levels in the blood.
The heart releases atrial natriuretic peptide (ANP) to help regulate salt and water balance. When cells in the atria are stretched from excess blood volume, they release ANP. This hormone promotes excretion of sodium and therefore increases urine volume. This effect is functionally antagonistic to aldosterone because it lowers blood volume and pressure, and has no effect on blood osmolarity.
The thymus, located directly behind the sternum, releases thymosin, which is important for proper T-cell development and differentiation. The thymus atrophies by adulthood, and thymosin levels drop accordingly. The function of T-cells is discussed in Chapter 8 of MCAT Biology Review.
A full list of hormones and their actions can be found in Table 5.1 below.
Table 5.1 Major Hormones in Humans
SOURCE HORMONE TYPE ACTION
Anterior pituitary Follicle-stimulating hormone (FSH) Peptide Stimulates follicle maturation in females; spermatogenesis in males
Luteinizing hormone (LH) Peptide Stimulates ovulation in females; testosterone synthesis in males
Adrenocorticotropic hormone (ACTH) Peptide Stimulates the adrenal cortex to synthesize and secrete glucocorticoids
Thyroid-stimulating hormone (TSH) Peptide Stimulates the thyroid to produce thyroid hormones
Prolactin Peptide Stimulates milk production and secretion
Endorphins Peptide Decrease sensation of pain; can promote euphoria
Growth hormone (GH) Peptide Stimulates bone and muscle growth; raises blood glucose levels
Hypothalamus (released by posterior pituitary) Antidiuretic hormone (ADH; vasopressin) Peptide Stimulates water reabsorption in kidneys by increasing permeability of collecting duct
Oxytocin Peptide Stimulates uterine contractions during labor and milk secretion during lactation; may promote bonding behavior
Thyroid (follicular cells) Triiodothyronine (T3) and thyroxine (T4) Amino acid–derivative Stimulate metabolic activity
Thyroid (parafollicular or C cells) Calcitonin Peptide Decreases blood calcium concentrations
Parathyroids Parathyroid hormone (PTH) Peptide Increases blood calcium concentrations
Adrenal cortex Glucocorticoids (cortisol and cortisone) Steroid Increase blood glucose concentrations; decrease protein synthesis; anti-inflammatory
Mineralocorticoids (aldosterone) Steroid Increase water reabsorption in the kidneys by increasing sodium reabsorption; promote potassium and hydrogen ion excretion
Adrenal medulla Epinephrine and norepinephrine Amino acid–derivative Increase blood glucose concentrations and heart rate; dilate bronchi; alter blood flow patterns
Pancreas (α-cells) Glucagon Peptide Stimulates glycogen breakdown (glycogenolysis); increases blood glucose concentrations
Pancreas (β-cells) Insulin Peptide Lowers blood glucose concentrations and promotes anabolic processes
Pancreas (δ-cells) Somatostatin Peptide Suppresses secretion of glucagon and insulin
Testis (and adrenal cortex) Testosterone Steroid Induces the development and maintenance of male reproductive system and male secondary sex characteristics
Ovary (and placenta) Estrogen Steroid Induces the development and maintenance of female reproductive system and female secondary sex characteristics
Progesterone Steroid Promotes maintenance of the endometrium
Pineal gland Melatonin Peptide Involved in circadian rhythms
Kidney Erythropoietin Peptide Stimulates bone marrow to produce erythrocytes
Heart (atria) Atrial natriuretic peptide (ANP) Peptide Promotes salt and water excretion
Thymus Thymosin Peptide Stimulates T-cell development
MCAT CONCEPT CHECK 5.2
Before you move on, assess your understanding of the material with these questions.
- For each of the hypothalamic releasing hormones listed below, what hormone(s) does each affect in the anterior pituitary? On which organ does each pituitary hormone act? What hormone(s) are released by the target organs?
Hypothalamic Releasing Hormone Hormone(s) from Anterior Pituitary Target Organ Hormone(s) Released by Target Organ
Gonadotropin-releasing hormone (GnRH) Corticotropin-releasing factor (CRF) Thyroid-releasing hormone (TRH) Dopamine
N/A
Growth hormone–releasing hormone (GHRH)
N/A
- Which two hormones are primarily involved in calcium homeostasis? Where does each come from, and what effect does each have on blood calcium concentrations?
-
-
- Which endocrine tissue synthesizes catecholamines? What are the two main catecholamines it produces?
- Which two pancreatic hormones are the major drivers of glucose homeostasis? Where does each come from, and what effect does each have on blood glucose concentrations?
-
-
- Which three hormones are primarily involved in water homeostasis? Where does each come from, and what effect does each have on blood volume and osmolarity?
-
-
-
Conclusion
The endocrine system is unique because its organs are not anatomically related. Hormones are produced in a wide variety of locations and can have far-reaching effects throughout the entire organism. The endocrine system allows for integration and execution of the homeostatic parameters that are necessary to ensure proper functioning of the body. For example, we learned that calcium levels are maintained within a narrow concentration range in the plasma by the antagonistic actions of calcitonin and parathyroid hormone (and vitamin D). Each hormone manipulates the steady state of the organism. As you continue your study of the human body, you will find that the endocrine system has effects on every system of the body by regulating fuel metabolism, blood flow, growth, and development.
In the last section of this chapter, there was a small note on erythropoietin, the hormone that stimulates the production of red blood cells in the bone marrow. Don’t interpret this brief mention as an indication that it is relatively unimportant. In fact, every cell of the body (except red blood cells themselves) needs a constant supply of oxygen to accomplish its function. Our bodies take in this oxygen through the respiratory system and then distribute the oxygen to tissues via the circulatory system. In the next two chapters, we will explore each of these systems separately. Recognize, however, that this division is artificial; indeed, like the body as a whole, the respiratory and circulatory systems are inseparable as they serve a common function: providing oxygen for every working cell in the body.
GO ONLINE
You've reviewed the content, now test your knowledge and critical thinking skills by completing a test-like passage set in your online resources!
CONCEPT SUMMARY
Mechanisms of Hormone Action
- Endocrine signaling involves the secretion of hormones directly into the bloodstream. The hormones travel to distant target tissues, where they bind to receptors and induce a change in gene expression or cell function.
- Peptide hormones are composed of amino acids and are derived from larger precursor proteins that are cleaved during posttranslational modification.
- Peptide hormones are polar and cannot pass through the plasma membrane.
- These hormones bind to extracellular receptors, where they trigger the transmission of a second messenger.
- Each step of the signaling cascade can induce amplification of the signal.
- Peptide hormones exert effects that usually have rapid onset but are short lived.
- These hormones are water-soluble, so they travel freely in the bloodstream and do not require a special carrier.
- Steroid hormones are derived from cholesterol.
- Steroid hormones are minimally polar and can pass through the plasma membrane.
- These hormones bind to and promote a conformational change in cytosolic or intranuclear receptors; the hormone–receptor complex binds to DNA, altering the transcription of a particular gene.
- Steroid hormones exert effects that usually have slow onset but are long-lived.
- Because these hormones are lipid-soluble, they cannot dissolve in the bloodstream and must be carried by specific proteins.
- Amino acid–derivative hormones are modified amino acids.
- Their chemistry shares some features with peptide hormones and some features with steroid hormones; different amino acid–derivative hormones share different features with these other hormone classes.
- Common examples are epinephrine, norepinephrine, triiodothyronine, and thyroxine.
- Hormones can be classified by their target tissues.
- Direct hormones have major effects on non-endocrine tissues.
- Tropic hormones have major effects on other endocrine tissues.
Endocrine Organs and Hormones
- The hypothalamus is the bridge between the nervous and endocrine systems.
- The release of hormones from the hypothalamus is mediated by a number of factors, including projections from other parts of the brain, chemo- and baroreceptors in the blood vessels, and negative feedback from other hormones.
- In negative feedback, the final hormone (or product) of a pathway inhibits hormones (or enzymes) earlier in the pathway, maintaining homeostasis.
- The hypothalamus stimulates the anterior pituitary gland through paracrine release of hormones into the hypophyseal portal system, which directly connects the two organs.
- Gonadotropin-releasing hormone (GnRH) promotes the release of follicle-stimulating hormone (FSH) and luteinizing hormone (LH).
- Growth hormone–releasing hormone (GHRH) promotes the release of growth hormone.
- Thyroid-releasing hormone (TRH) promotes the release of thyroid-stimulating hormone (TSH).
- Corticotropin-releasing factor (CRF) promotes the release of adrenocorticotropic hormone (ACTH).
- Prolactin-inhibiting factor (PIF or dopamine) inhibits the release of prolactin.
- Interactions with the posterior pituitary occur via the axons of nerves projected by the hypothalamus. Antidiuretic hormone (ADH or vasopressin) and oxytocin are synthesized in the hypothalamus and then travel down these axons to the posterior pituitary, where they are released into the bloodstream.
- The anterior pituitary releases hormones in response to stimulation from the hypothalamus. Four of these (FSH, LH, ACTH, and TSH) are tropic hormones, while three (prolactin, endorphins, and growth hormone) are direct hormones.
- Follicle-stimulating hormone (FSH) promotes the development of ovarian follicles in females and spermatogenesis in males.
- Luteinizing hormone (LH) promotes ovulation in females and testosterone production in males.
- Adrenocorticotropic hormone (ACTH) promotes the synthesis and release of glucocorticoids from the adrenal cortex.
- Thyroid-stimulating hormone (TSH) promotes the synthesis and release of triiodothyronine and thyroxine from the thyroid.
- Prolactin promotes milk production.
- Endorphins decrease perception of pain and can produce euphoria.
- Growth hormone (GH) promotes growth of bone and muscle and shunts glucose to these tissues. It raises blood glucose concentrations.
- The posterior pituitary releases two hormones produced in the hypothalamus.
- Antidiuretic hormone (ADH or vasopressin) is secreted in response to low blood volume or increased blood osmolarity and increases reabsorption of water in the collecting duct of the nephron, increasing blood volume and decreasing blood osmolarity.
- Oxytocin is secreted during childbirth and promotes uterine contractions. It also promotes milk ejection and may be involved in bonding behavior. It is unusual in that it has a positive feedback loop, not negative.
- The thyroid is located at the base of the neck in front of the trachea; it produces three key hormones.
- Triiodothyronine (T3) and thyroxine (T4) are produced by follicular cells and contain iodine. They increase basal metabolic rate and alter the utilization of glucose and fatty acids. Thyroid hormones are required for proper neurological and physical development in children.
- Calcitonin is produced by parafollicular (C) cells. It decreases plasma calcium concentration by promoting calcium excretion in the kidneys, decreasing calcium absorption in the gut, and promoting calcium storage in bone.
- The parathyroid glands release parathyroid hormone (PTH), which increases blood calcium concentration.
- PTH decreases excretion of calcium by the kidneys and increases bone resorption directly to increase blood calcium concentration.
- PTH activates vitamin D, which is necessary for calcium and phosphate absorption from the gut.
- PTH promotes resorption of phosphate from bone and reduces reabsorption of phosphate in the kidney, but vitamin D promotes absorption of phosphate from the gut; these two effects on phosphate concentration somewhat cancel each other out.
- The adrenal cortex produces three classes of steroid hormones.
- Glucocorticoids such as cortisol and cortisone increase blood glucose concentration, reduce protein synthesis, inhibit the immune system, and participate in the stress response. Glucocorticoid release is stimulated by ACTH.
- Mineralocorticoids such as aldosterone promote sodium reabsorption in the distal convoluted tubule and collecting duct, thus increasing water reabsorption. Aldosterone also increases potassium and hydrogen ion excretion. Aldosterone activity is regulated by the renin–angiotensin–aldosterone system, not ACTH.
- Cortical sex hormones include androgens (like testosterone) and estrogens in both males and females.
- The adrenal medulla is derived from the nervous system and secretes catecholamines into the bloodstream.
- Catecholamines include epinephrine and norepinephrine, which are involved in the fight-or-flight (sympathetic) response.
- These hormones promote glycogenolysis, increase the basal metabolic rate, increase heart rate, dilate the bronchi, and alter blood flow.
- The endocrine pancreas produces hormones that regulate glucose homeostasis.
- Glucagon is produced by α-cells and raises blood glucose levels by stimulating protein and fat degradation, glycogenolysis, and gluconeogenesis.
- Insulin is produced by β-cells and lowers blood glucose levels by stimulating glucose uptake by cells and promoting anabolic processes, like glycogen, fat, and protein synthesis.
- Somatostatin is produced by δ-cells and inhibits insulin and glucagon secretion.
- The gonads produce hormones that are involved in the development and maintenance of the reproductive systems and secondary sex characteristics.
- The testes secrete testosterone.
- The ovaries secrete estrogen and progesterone.
- The pineal gland releases melatonin, which helps to regulate circadian rhythms.
- Other organs may release hormones, even if they are not primarily considered part of the endocrine system.
- Cells in the stomach and intestine produce hormones like secretin, gastrin, and cholecystokinin.
- The kidneys secrete erythropoietin, which stimulates bone marrow to produce erythrocytes (red blood cells) in response to low oxygen levels in the blood.
- The atria of the heart secrete atrial natriuretic peptide (ANP), which promotes excretion of salt and water in the kidneys in response to stretching of the atria (high blood volume).
- The thymus secretes thymosin, which is important for proper T-cell development and differentiation.
ANSWERS TO CONCEPT CHECKS
**5.1**
-
Criterion Peptide Hormones Steroid Hormones
Chemical precursor Amino acids (polypeptides) Cholesterol
Location of receptor Extracellular (cell membrane) Intracellular or intranuclear
Mechanism of action Stimulates a receptor (usually a G protein–coupled receptor), affecting levels of second messengers (commonly cAMP). Initiates a signal cascade Binds to a receptor, induces conformational change, and regulates transcription at the level of the DNA
Method of travel in the bloodstream Dissolves and travels freely Binds to a carrier protein
Speed of onset Quick Slow
Duration of action Short lived Long lived
- Amino acid–derivative hormones are made by modifying amino acids, such as the addition of iodine to tyrosine (in thyroid hormone production).
- Direct hormones are secreted into the bloodstream and travel to a target tissue, where they have direct effects. Tropic hormones cause secretion of another hormone that then travels to the target tissue to cause an effect.
**5.2**
-
Hypothalamic Releasing Hormone Hormone(s) from Anterior Pituitary Target Organ Hormone(s) Released by Target Organ
Gonadotropin-releasing hormone (GnRH) Follicle-stimulating hormone (FSH) and luteinizing hormone (LH) Gonads (testes or ovaries) Testosterone (testes) or estrogen and progesterone (ovaries)
Corticotropin-releasing factor (CRF) Adrenocorticotropic hormone (ACTH) Adrenal cortex Glucocorticoids (cortisol and cortisone)
Thyroid-releasing hormone (TRH) Thyroid-stimulating hormone (TSH) Thyroid Triiodothyronine (T3), thyroxine (T4)
Dopamine Prolactin* Breast tissue N/A
Growth hormone–releasing hormone (GHRH) Growth hormone Bone, muscle N/A
Note that adecrease* in dopamine from the hypothalamus promotes prolactin secretion.
- Calcitonin from the parafollicular (C-) cells of the thyroid decreases blood calcium concentration. Parathyroid hormone from the parathyroid glands increases blood calcium concentration.
- The adrenal medulla synthesizes catecholamines, including epinephrine and norepinephrine.
- Glucagon from the α-cells of the pancreas increases blood glucose concentration. Insulin from the β-cells of the pancreas decreases blood glucose concentration.
- Antidiuretic hormone (ADH or vasopressin) from the hypothalamus (released by the posterior pituitary) increases blood volume and decreases blood osmolarity. Aldosterone from the adrenal cortex increases blood volume with no effect on blood osmolarity. Atrial natriuretic peptide (ANP) from the heart decreases blood volume with no effect on blood osmolarity.
SCIENCE MASTERY ASSESSMENT EXPLANATIONS
1. C
Unlike the other hormones listed here, ADH is not secreted by the adrenal cortex and is therefore not a –corticoid. Rather, ADH is a peptide hormone produced by the hypothalamus and released by the posterior pituitary that promotes water reabsorption. The other associations are all correct.
2. D
A hormone that directly stimulates a non-endocrine target tissue is referred to as a direct hormone. Glancing at the answer choices, we notice that all of the hormones are secreted by the anterior pituitary gland. The direct hormones secreted by the anterior pituitary are prolactin, endorphins, and growth hormone (GH). All of the other answer choices are tropic hormones. The tropic hormones of the anterior pituitary include follicle-stimulating hormone (FSH), luteinizing hormone (LH), adrenocorticotropic hormone (ACTH), and thyroid-stimulating hormone (TSH).
3. A
The parathyroid glands secrete parathyroid hormone (PTH), a hormone that functions to increase blood calcium levels. An increase in synthetic activity of the parathyroid glands would lead to an increase in PTH and, therefore, an increase in blood calcium levels through three mechanisms: increased calcium reabsorption in the kidneys (decreased excretion), increased bone resorption, and increased absorption of calcium from the gut (via activation of vitamin D).
4. B
Peptide hormones are composed of chains of amino acids and, though they vary in size, are generally too large, charged, and polar to cross the cell membrane. Instead, these hormones bind to extracellular receptors and rely on second messengers to mediate their effects. All of these observations justify (B).
5. B
Inflammation of the thyroid or iodine deficiency can cause hypothyroidism, in which the thyroid hormones are undersecreted or not secreted at all. Hypothyroidism in newborn infants causes cretinism, which is characterized by poor neurological and physical development (including intellectual disabilities, short stature, and coarse facial features). While iodine deficiency can result in a swelling of the thyroid gland (called a goiter), which can also be seen in causes of hyperthyroidism, iodine deficiency does not cause hyperthyroidism, eliminating(D). Galactorrhea,(A), is associated with prolactin; gigantism,(C), is associated with growth hormone.
6. C
The hypothalamic–pituitary–thyroid axis includes the secretion of thyroid-releasing hormone (TRH) from the hypothalamus triggering the secretion of thyroid-stimulating hormone (TSH) from the anterior pituitary, which stimulates the secretion of triiodothyronine (T3) and thyroxine (T4) from the thyroid. Overproduction of TRH would promote overproduction of TSH, eliminating (B). Destruction of the follicular cells that produce T3 and T4 would remove negative feedback, allowing TSH levels to rise, eliminating (A) and (D). High levels of T4 would cause too much negative feedback and lower TSH levels, making (C)the correct answer.
7. B
Steroid hormones are nonpolar cholesterol derivatives and bind to internal receptors. Importantly, as cholesterol derivatives, these hormones generally lack nitrogen and are composed primarily of carbon, hydrogen, and oxygen. All of these factors support (B) as the right answer. By contrast, (A) can be eliminated because peptide hormones would localize to the cell surface. And, while amino acid derivatives can signal like steroid hormones, (C) can be eliminated since the chemical composition given in the question stem indicates a lack of nitrogen. (D) can be eliminated since the term "direct" refers to the hormone target, and data about the target of the hormone are not given in this question stem.
8. B
Pancreatic somatostatin secretion is increased by high blood glucose or amino acid levels, leading to decreased insulin and glucagon secretion, eliminating (A) and (D). Somatostatin is thus always an inhibitory hormone, confirming (B). The stimuli for somatostatin release include high blood glucose or amino acids, as mentioned above, as well as high levels of certain gastrointestinal hormones, as discussed in Chapter 9 of MCAT Biology Review—but not cortisol, eliminating (C).
9. C
β-cells are responsible for insulin production. The function of insulin is to lower blood glucose levels by promoting the influx of glucose into cells and by stimulating anabolic processes, such as glycogenesis or fat and protein synthesis. Thus, destruction of the β-cells would result in a cessation of insulin production, which would lead to hyperglycemia, or high blood glucose concentration.
10. D
The stimulus for renin production is low blood pressure, which causes the juxtaglomerular cells of the kidney to produce renin, an enzyme that converts the plasma protein angiotensinogen to angiotensin I. Angiotensin I is then converted to angiotensin II by an enzyme in the lungs; angiotensin II then stimulates the adrenal cortex to secrete aldosterone. Aldosterone helps to restore blood volume by increasing sodium reabsorption in the kidney, leading to an increase in water reabsorption. This removes the initial stimulus for renin production. Thus, (A), (B), and (C)correctly describe the renin–angiotensin–aldosterone system, while (D) describes the stimulus for erythropoietin secretion.
11. B
The question stem indicates that the newly discovered hormone functions as a first messenger, stimulating the conversion of ATP to cAMP; cAMP functions as a second messenger, triggering a signaling cascade in the cell. Hormones that act via second messengers and are relatively large in size (short peptides or complex polypeptides) are peptide hormones. This hormone could be a tropic hormone, but it is also entirely possible for it to be a direct hormone; thus, (D)can be eliminated.
12. B
Regardless of the cause, the low levels of calcium in the blood require treatment. While other therapies are more frequently used to treat hypocalcemia (low blood calcium levels), such as calcium gluconate or calcium chloride, administration of parathyroid hormone would also raise blood calcium concentration. Calcitonin would be a poor choice in this case, as this hormone lowers blood calcium concentrations, eliminating (A). Aldosterone and thymosin play no role in calcium homeostasis, eliminating (C)and (D).
13. C
Both oxytocin and vasopressin (another name for antidiuretic hormone) end with the suffix –in; this should hint that they are peptide or amino acid–derivative hormones. These two hormones are both synthesized by the hypothalamus, but released by the posterior pituitary. Remember that the posterior pituitary does not actually synthesize any hormones itself; rather, it contains the axons that originate in cells in the hypothalamus and is the site of release for these hormones.
14. C
Dopamine is used in a number of neurological systems; most relevant to the endocrine system is the fact that dopamine secretion prevents prolactin release. Thus, an individual taking medications that block dopamine receptors would lose this inhibition on prolactin release and have elevated prolactin levels.
15. D
The question stem states that an infant who is genotypically female is born with ambiguous genitalia, meaning that the genitalia do not appear to be specifically female or specifically male. In a genotypic female, this indicates that the infant was exposed to androgens during the fetal period. In addition, the infant is also losing sodium, causing hyponatremia. This indicates two issues: excess androgens and a lack of aldosterone, a hormone required for proper reuptake of sodium in the kidneys. Both of these hormones are synthesized in the adrenal cortex, making (D)the correct answer. Note that neither of these hormones is regulated by the hypothalamic–pituitary–adrenal axis, eliminating (A) and (B).
GO ONLINE
Consult your online resources for additional practice.
SHARED CONCEPTS
Behavioral Sciences Chapter 5
Motivation, Emotion, and Stress
Biochemistry Chapter 3
Nonenzymatic Protein Function and Protein Analysis
Biochemistry Chapter 8
Biological Membranes
Biochemistry Chapter 12
Bioenergetics and Regulation of Metabolism
Biology Chapter 4
The Nervous System
Biology Chapter 10
Homeostasis