Chapter 9: The Digestive System
Chapter 9: The Digestive System
SCIENCE MASTERY ASSESSMENT
Every pre-med knows this feeling: there is so much content I have to know for the MCAT! How do I know what to do first or what's important?
While the high-yield badges throughout this book will help you identify the most important topics, this Science Mastery Assessment is another tool in your MCAT prep arsenal. This quiz (which can also be taken in your online resources) and the guidance below will help ensure that you are spending the appropriate amount of time on this chapter based on your personal strengths and weaknesses. Don't worry though— skipping something now does not mean you'll never study it. Later on in your prep, as you complete full-length tests, you'll uncover specific pieces of content that you need to review and can come back to these chapters as appropriate.
How to Use This Assessment
If you answer 0–7 questions correctly:
Spend about 1 hour to read this chapter in full and take limited notes throughout. Follow up by reviewing all quiz questions to ensure that you now understand how to solve each one.
If you answer 8–11 questions correctly:
Spend 20–40 minutes reviewing the quiz questions. Beginning with the questions you missed, read and take notes on the corresponding subchapters. For questions you answered correctly, ensure your thinking matches that of the explanation and you understand why each choice was correct or incorrect.
If you answer 12–15 questions correctly:
Spend less than 20 minutes reviewing all questions from the quiz. If you missed any, then include a quick read-through of the corresponding subchapters, or even just the relevant content within a subchapter, as part of your question review. For questions you answered correctly, ensure your thinking matches that of the explanation and review the Concept Summary at the end of the chapter.
- Which of the following associations correctly matches a gastric cell with a compound it secretes?
- G-cells—HCl
- Chief cells—pepsinogen
- Parietal cells—alkaline mucus
- Mucous cells—intrinsic factor
- Which of the following is NOT part of the small intestine?
- Ileum
- Cecum
- Jejunum
- Duodenum
- In an experiment, enteropeptidase secretion was blocked. As a direct result, levels of all of the following active enzymes would likely be affected EXCEPT:
- trypsin.
- aminopeptidase.
- chymotrypsin.
- carboxypeptidase A.
- Which of the following INCORRECTLY pairs a digestive enzyme with its function?
- Trypsin—hydrolyzes specific peptide bonds
- Lactase—hydrolyzes lactose to glucose and galactose
- Pancreatic amylase—hydrolyzes starch to maltose
- Lipase—emulsifies fats
- Which of the following correctly lists two organs in which proteins are digested?
- Mouth and stomach
- Stomach and large intestine
- Stomach and small intestine
- Small intestine and large intestine
- Which of the following choices INCORRECTLY pairs a digestive enzyme with its site of secretion?
- Sucrase—salivary glands
- Carboxypeptidase—pancreas
- Trypsin—pancreas
- Lactase—duodenum
- A two-week-old infant is brought to the emergency room. The infant’s caregiver reports that the infant has been unable to keep any milk down; shortly after nursing, the infant has sudden projectile vomiting. During exam, an olive-shaped mass can be felt in the infant’s upper abdomen. It is determined that there is a constriction in the digestive system that prevents food from reaching the small intestine from the stomach. Which structure is most likely the site of the problem?
- Cardiac sphincter
- Pyloric sphincter
- Ileocecal valve
- Internal anal sphincter
- Many medications have anticholinergic side effects, which block the activity of parasympathetic neurons throughout the body. Individuals who are older may be on many such medications simultaneously, exacerbating the side effects. Which of the following would NOT be expected in an individual taking medications with anticholinergic activity?
- Dry mouth
- Diarrhea
- Slow gastric emptying
- Decreased gastric acid production
- The two graphs below show the relative activities of two enzymes in solutions of varying pH. Which of the following choices correctly identifies the two enzymes?
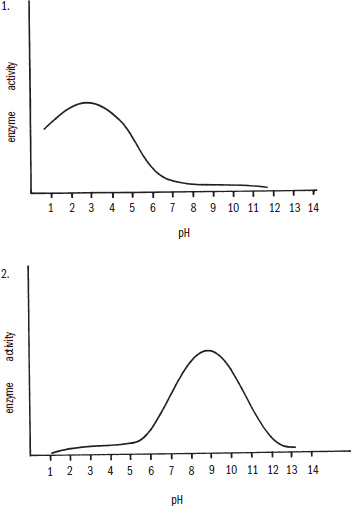
- 1—chymotrypsin; 2—pepsin
- 1—pepsin; 2—carboxypeptidase B
- 1—lactase; 2—aminopeptidase
- 1—enteropeptidase; 2—amylase
- Which of the following would NOT likely lead to elevated levels of bilirubin in the blood?
- Cholangiocarcinoma, a cancer of the bile ducts that can ultimately lead to full occlusion of the duct lumen
- Autoimmune hemolytic anemia, a disease in which the red blood cells are attacked by antibodies and are lysed
- Ménétrier’s disease, in which rugae thicken and overlying glands lose secretory ability
- Acetaminophen (Tylenol) overdose, in which the accumulation of toxic metabolites can cause rapid liver failure
- Which of the following correctly pairs the molecule with its primary site of absorption?
- Chylomicrons—lacteals
- Amino acids—large intestine
- Vitamins A and E—stomach
- Cholesterol—ascending colon
- The cleavage of fats into glycerol and fatty acids catalyzed by lipases in the lumen of the duodenum is best described as:
- mechanical digestion.
- chemical digestion.
- intracellular digestion.
- absorption.
- Which of the following biomolecules does NOT drain into the liver before arriving at the right side of the heart?
- Cholecalciferol (vitamin D)
- Threonine (an amino acid)
- Fructose (a monosaccharide)
- Pantothenic acid (vitamin B5)
- Which of the following hormones increases feeding behavior?
- Leptin
- Cholecystokinin
- Ghrelin
- Gastrin
- Which of the following is likely to be seen in a patient with liver failure?
- High concentrations of urea in the blood
- High concentrations of albumin in the blood
- Low concentrations of ammonia in the blood
- Low concentrations of clotting factors in the blood
Answer Key
- B
- B
- B
- D
- C
- A
- B
- B
- B
- C
- A
- B
- A
- C
- D
Chapter 9: The Digestive System
CHAPTER 9
THE DIGESTIVE SYSTEM
In This Chapter
9.1 Anatomy of the Digestive System 9.2 Ingestion and Digestion
Oral Cavity
Pharynx
Esophagus
Stomach
Duodenum
9.3 Accessory Organs of Digestion
Pancreas
Liver
Gallbladder
9.4 Absorption and Defecation
Jejunum and Ileum
Large Intestine
Concept Summary
CHAPTER PROFILE
The content in this chapter should be relevant to about 4% of all questions about biology on the MCAT.
This chapter covers material from the following AAMC content category:
3B: Structure and integrative functions of the main organ systems
Introduction
As we continue our survey of organ systems, we now come to the digestive system. As with our previous reviews of other organ systems, we will start with a basic anatomical overview of the organs of digestion (including the accessory organs) and then move on to discuss how these organs function to provide nutrition to the individual. The food we eat is complex, incorporating meats, grains, vegetables and fruits, dairy products, and nuts. The job of the digestive system is to take these complex foods—composed of polysaccharides, fats, and proteins—and turn large macromolecules into smaller, simpler monosaccharides, fatty acids, and amino acids. In order to cleave all of these bonds, the body requires a complex system of mechanical and chemical agents. These compounds can then be absorbed from the gut, transported to the tissues by the circulatory system, and used by cells. In this chapter, we will consider the organs that make up the digestive system as well as the processes by which the foods we eat become the fuel we need for energy, growth, development, and maintenance of other essential activities.
9.1 Anatomy of the Digestive System
LEARNING OBJECTIVES
After Chapter 9.1, you will be able to:
- Describe mechanical and chemical digestion and differentiate between them
- Identify the interactions between the sympathetic and parasympathetic nervous systems and the digestive system
- Trace the path of food through the body, naming major organs and valves in the digestive tract
There are two types of digestion that occur. First, intracellular digestion, as a part of metabolism, involves the oxidation of glucose and fatty acids for energy. However, our diets do not consist of pure glucose and fatty acids; rather, these substances must be extracted from our food. The process by which these nutrients are obtained from food occurs within the lumen of the alimentary canal and is known as extracellular digestion. This is technically “outside” the body, because the lumen of the gastrointestinal tract communicates directly with the outside world. The alimentary canal runs from the mouth to the anus and is sectioned off by sphincters, or circular smooth muscles around the canal that can contract to allow compartmentalization of function.
The human digestive tract has specialized sections with different functional roles. The most basic functional distinction is between digestion and absorption. Digestion involves the breakdown of food into its constituent organic molecules: starches and other carbohydrates into monosaccharides, lipids (fats) into free fatty acids and glycerol, and proteins into amino acids. Digestion can be subdivided into mechanical and chemical processes. Mechanical digestion is the physical breakdown of large food particles into smaller food particles, but does not involve breaking chemical bonds. Chemical digestion is the enzymatic cleavage of chemical bonds, such as the peptide bonds of proteins or the glycosidic bonds of starches. Absorption involves the transport of products of digestion from the digestive tract into the circulatory system for distribution to the body’s tissues and cells.
The digestive tract, shown in Figure 9.1, begins with the oral cavity (mouth) followed by the pharynx, a shared pathway for both food entering the digestive system and air entering the respiratory system. From the pharynx, food enters the esophagus, which transports it to the stomach. From the stomach, food travels to the small intestine, and then to the large intestine. Finally, waste products of digestion enter the rectum, where feces are stored until an appropriate time of release. In addition to the digestive tract itself, the salivary glands, pancreas, liver, and gallbladder help to provide the enzymes and lubrication necessary to aid in the digestion of food.
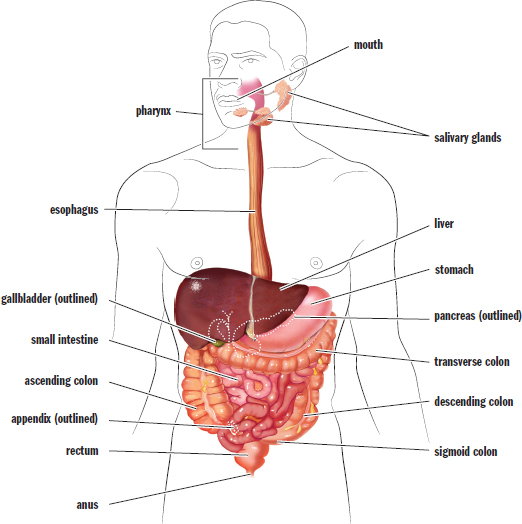
Figure 9.1. Anatomy of the Digestive System
The enteric nervous system is a collection of one hundred million neurons that govern the function of the gastrointestinal system. These neurons are present in the walls of the digestive tract and trigger peristalsis, or rhythmic contractions of the gut tube, in order to move materials through the system. This system can function independently of the brain and spinal cord, although it is heavily regulated by the autonomic nervous system. The parasympathetic division is involved in stimulation of digestive activities, increasing secretions from exocrine glands and promoting peristalsis. The sympathetic division is involved in the inhibition of these activities. The fact that so often we feel sleepy and lethargic after eating a big meal (often called a food coma colloquially) is due, in part, to parasympathetic activity. On the other hand, during periods of high sympathetic activity, bloodflow is decreased to the digestive tract, and gut motility slows significantly.
KEY CONCEPT
All of the glands of the body (except sweat glands) are innervated by the parasympathetic nervous system.
BIOLOGY GUIDED EXAMPLE WITH EXPERT THINKING
Bile acids are crucial for the intestinal absorption of dietary fatty acids, of cholesterol, and of fat-soluble vitamins. To determine whether the interruption of the enterohepatic circulation of bile acids alters triglyceride and glucose metabolism, researchers tested ileal sodium-dependent bile acid transporter (Slc10a2) KO mice. Over 95% of intestinal bile acid is absorbed and returned to the liver; thus, knocking out Slc10a2 should dramatically reduce the total pool of bile acid in the body (approx. 80% reduction). In addition, some mice were fed a sucrose-rich (SR) diet to simulate the metabolic stress of an unhealthy diet. *This is just background information Purpose: determine whether removing bile acids changes metabolism
A new abbreviation "KO" is here, but the next sentence says “knocking out”, so I know this must stand for “Knock Out” This details the IVs: normal vs reduced bile acids and regular vs sugary diet*
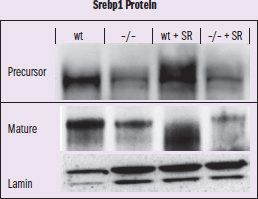
Figure 1 Expression of sterol regulatory element-binding protein 1 (Srebp1) Protein Immunoblot. The transcription factor Srebp1c is crucial for optimal activation of most genes in fatty acid synthesis and gluconeogensis. WT is wild-type and –/– is the KO, so SR must be the diet IV: Srebp1 in WT, KO, with and without SR DV: expression of precursor and mature protein Trends: WT mice with SR have increased levels of protein; there is no noticeable change for KO mice with or without SR This is testing for a new protein involved in fatty acid synthesis and gluconeogenesis (metabolic protein)
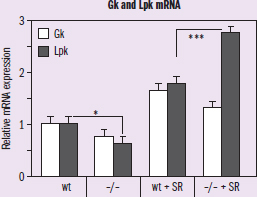
Figure 2 Hepatic mRNA expression of Glucokinase (Gk) and Liver Pyruvate Kinase (Lpk) IVs: Gk and Lpk in WT and KO with and without diet (SR) DV: relative mRNA expression Trend: Lpk is signficantly lower in KO mice without the diet and significantly higher in KO mice with the diet
Adapted from Lundåsen T, Andersson E-M, Snaith M, Lindmark H, Lundberg J, Östlund-Lindqvist A-M, et al. (2012) Inhibition of intestinal bile acid transporter slc10a2 improves triglyceride metabolism and normalizes elevated plasma glucose levels in mice. PLoS One 7(5): e37787. https://doi.org/10.1371/journal.pone.0037787.
Would reducing the total pool of bile acid be a good strategy to combat the hypertriglyceridemia and diabetes induced by an unhealthy diet?
This question asks whether an action, reducing the total pool of bile acid, would have a specified impact on two conditions, hypertriglyceridemia and diabetes. To answer this question, we must assess the data we are given in the article regarding how changing bile acid quantity affects traits and outcomes associated with those conditions.
We should start by making sure we‘re comfortable with the terms used in the question, relying on either the article or our critical thinking skills to fill our knowledge gaps. Hypertriglyceridemia is a condition when blood triglyceride levels are too high, and diabetes is a condition when blood glucose levels are too high. However, that information wasn’t given to us in the passage, and it‘s not entirely in scope for Test Day—so how could we figure out what we need to know to answer this question? Even if we didn’t know this, though, we know the mice were fed food to simulate an unhealthy diet that would supply them with too much sugar, and we should recognize at least diabetes as a metabolic disorder linked with sugar metabolism. We should also recognize that triglycerides are fats, so this is probably a condition involving fat metabolism. Thus, we can assume that any action that lowers blood triglycerides (relating to hypertriglyceridemia) and blood glucose (relating to diabetes) could constitute a potentially beneficial therapy for these two conditions. So, when we look at the data for the experimental mice as compared to controls, we should be looking for changes related to these two metabolic pathways to determine if there are possible treatment implications for reducing bile salt concentrations in order to treat these conditions.
According to the passage, the knockout mice do not have the bile acid transporter, meaning that the pool of available bile acid in their system should be significantly lower. There's also a second variable, diet, which should be simulating mice that are experiencing metabolic stressors in the sucrose-rich condition as compared to normal metabolic function. Figure 1 shows the concentration of a protein involved in fatty acid synthesis in the KO mice versus wild-type mice, with both normal and sucrose-rich diets. In the wild-type mice, we can see that the addition of a metabolically stressful, high-sugar diet (lane 3) leads to a big increase in production of that protein as compared to regular diet (lane 1). However, in the knockout mice, there’s no perceivable change from the regular diet (lane 2) to the sucrose-rich diet (lane 4). This is true both for the actual protein and the precursor, which means that the KO mouse is just not transcribing as much of that metabolic protein. The lamin lane down at the bottom seems like it‘s just a control for protein expression, and it looks pretty much the same across the board, so we can ignore it in our data analysis. Based on this figure, which is all about a metabolic protein in the fatty acid synthesis chain, it looks like the knockout mice just aren’t experiencing the same amount of metabolic stress; they‘re not trying to turn that extra sucrose into fatty acids. Based on this piece of data, it looks like reducing bile acid might be one way to relieve the metabolic stress associated with hypertriglyceridemia, or at least, it’s worth more investigation!
Moving on, Figure 2 shows the same conditions, but is measuring mRNA production of two different proteins: glucokinase and pyruvate kinase. Even if we aren‘t exactly sure of what those enzymes do, they have glucose and pyruvate in their names, so it sounds like they are probably involved in the sugar metabolism pathway. Looking at the figure, we can see in the first two pairs of columns that wild-type mice are expressing more mRNA for both of these proteins than KO mice. After metabolic stress is added, it looks like pyruvate kinase production specifically spikes within the KO mice. That seems to indicate that these mice are responding to the metabolic stress to an even greater extent (in terms of Lpk) than the wild-type mice. Without directly measuring the level of blood glucose, we cannot determine whether that increased metabolic response represents a positive or negative trend. So, unlike the data in Figure 1, it looks like bile salt reduction may not be a good treatment option for diabetic individuals, and we may even need to reevaluate whether it would be truly helpful for those with triglyceridemia, as the energetic processing of fats can’t be considered as fully separate from the processing of sugars.
Overall, our takeaway is that we have mixed results. Figure 1 made the reduction of bile salts look like a promising treatment for triglyceridemia, but Figure 2 indicates that reducing bile salts may not be effective in treating diabetes. We can conclude that more data is needed to assess this therapy’s effect on sugar and lipid metabolism.
MCAT CONCEPT CHECK 9.1
Before you move on, assess your understanding of the material with these questions.
- What is the difference between mechanical and chemical digestion?
- Mechanical digestion:
- Chemical digestion:
- Trace the path of food through the body, starting with ingestion and ending with excretion of feces:
- What effect does the parasympathetic nervous system have on the digestive system? What effect does the sympathetic nervous system have?
- Parasympathetic nervous system:
- Sympathetic nervous system:
9.2 Ingestion and Digestion
LEARNING OBJECTIVES
After Chapter 9.2, you will be able to:
- Identify the secretory cells of the digestive tract, their secretions, and the function of their secretions
- Explain how bile and pancreatic lipase work together to digest fats
- Recall the key digestive enzymes and hormones produced in saliva, the stomach, and the intestines, and summarize the function of each
To supply the body with nutrients, we must ingest (eat) food. Several hormones are involved with feeding behavior, including antidiuretic hormone (ADH or vasopressin), aldosterone, glucagon, ghrelin, leptin, and cholecystokinin. ADH and aldosterone trigger the sensation of thirst, encouraging the behavior of fluid consumption. Glucagon, secreted by the pancreas, and ghrelin, secreted by the stomach and pancreas, stimulate feelings of hunger. Leptin and cholecystokinin do the opposite, stimulating feelings of satiety. Digestion begins in the oral cavity and continues in the stomach and the first part of the small intestine, known as the duodenum.
Oral Cavity
The oral cavity plays a role in both mechanical and chemical digestion of food. Mechanical digestion in the mouth involves the breaking up of large food particles into smaller particles using the teeth, tongue, and lips. This process is called mastication (chewing). Chewing helps to increase the surface area-to-volume ratio of the food, creating more surface area for enzymatic digestion as it passes through the gut tube. It also moderates the size of food particles entering the lumen of the alimentary canal; food particles that are too large create an obstruction risk in the tract.
KEY CONCEPT
The chemical digestion of carbohydrates occurs in both the mouth and small intestine, with the two amylases targeting complementary starches. Salivary amylase (active in the mouth) has a higher specificity for rapidly soluble starches, while pancreatic amylase (active in the small intestine) has a higher specificity for less soluble, more nonpolar starches.
Chemical digestion is the breakdown of chemical bonds in the macromolecules that make up food. This relies on enzymes from saliva produced by the three pairs of salivary glands. Saliva also aids mechanical digestion by moistening and lubricating food. The salivary glands, like all glands of the digestive tract, are innervated by the parasympathetic nervous system. The presence of food in the oral cavity triggers a neural circuit that ultimately leads to increased parasympathetic stimulation of these glands. Salivation can also be triggered by signals that food is near, such as smell or sight. Saliva contains salivary amylase, also known as ptyalin, and lipase. Salivary amylase is capable of hydrolyzing starch into smaller sugars (maltose and dextrins), while lipase catalyzes the hydrolysis of lipids. The amount of chemical digestion that occurs in the mouth is minimal, though, because the food does not stay in the mouth for long. Our muscular tongue forms the food into a bolus, which is forced back to the pharynx and swallowed.
REAL WORLD
There are three pairs of major salivary glands: the parotid, submandibular, and sublingual glands. Other microscopic salivary glands are scattered throughout the upper digestive system. While the parasympathetic nervous system is responsible for promoting salivation, the sympathetic nervous system has some input into the glands as well. The sympathetic nervous system increases the viscosity of saliva, which is why dry mouth and even a tacky sensation in the mouth occurs during a fight-or-flight response.
Pharynx
Thepharynx is the cavity that leads from the mouth and posterior nasal cavity to the esophagus. The pharynx connects not only to the esophagus, but also to the larynx, which is a part of the respiratory tract. The pharynx can be divided into three parts: the nasopharynx (behind the nasal cavity), the oropharynx (at the back of the mouth), and the laryngopharynx (above the vocal cords). Food is prevented from entering the larynx during swallowing by the epiglottis, a cartilaginous structure that folds down to cover the laryngeal inlet. Failure of this mechanism can lead to aspiration of food and choking.
Esophagus
Theesophagus is a muscular tube that connects the pharynx to the stomach. The top third of the esophagus is composed of skeletal muscle, the bottom third is composed of smooth muscle, and the middle third is a mix of both. What does this mean in terms of nervous control? While the top of the esophagus is under somatic (voluntary) motor control, the bottom—and most of the rest of the gastrointestinal tract, for that matter—is under autonomic (involuntary) nervous control. The rhythmic contraction of smooth muscle that propels food toward the stomach is called peristalsis. Under normal circumstances, peristalsis proceeds down the digestive tract. However, certain factors such as exposure to chemicals, infectious agents, physical stimulation in the posterior pharynx, and even cognitive stimulation, can lead to reversal of peristalsis in the process of emesis (vomiting).
Swallowing is initiated in the muscles of the oropharynx, which constitute the upper esophageal sphincter. Peristalsis squeezes, pushes, and propels the bolus toward the stomach. As the bolus approaches the stomach, a muscular ring known as the lower esophageal sphincter (cardiac sphincter) relaxes and opens to allow the passage of food.
REAL WORLD
Weakness in the lower esophageal sphincter is a key feature of gastroesophageal reflux disease (GERD), which causes classic heartburn symptoms after eating. As food and acid reflux into the lower esophagus, they irritate the less-protected mucosa, stimulating pain receptors. These receptors localize pain poorly, so a general burning sensation is felt in the lower chest—leading to the common term heartburn.
Stomach
There are three main energy sources: carbohydrates, fats, and proteins. As mentioned earlier, the chemical digestion of carbohydrates and fats is initiated in the mouth. No mechanical or chemical digestion takes place in the esophagus, except for the continued enzymatic activity initiated in the mouth by salivary enzymes. Thus, digestion that occurs prior to the entrance of the bolus into the stomach is minimal compared to the digestion that occurs in the stomach and small intestine.
The stomach is a highly muscular organ with a capacity of approximately two liters. In humans, the stomach is located in the upper left quadrant of the abdominal cavity, underneath the diaphragm. This organ uses hydrochloric acid and enzymes to digest food, creating a fairly harsh environment. Therefore, its mucosa is quite thick to prevent autodigestion. The stomach can be divided into four main anatomical divisions, as shown in Figure 9.2: the fundus and body, which contain mostly gastric glands, and the antrum and pylorus, which contain mostly pyloric glands. The internal curvature of the stomach is called the lesser curvature; the external curvature is called the greater curvature. The lining of the stomach is thrown into folds called rugae.
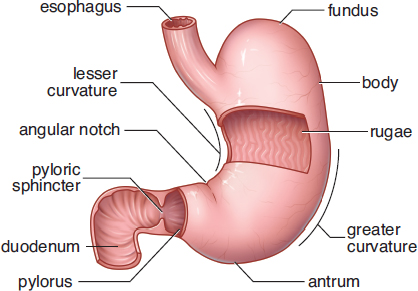
Figure 9.2. Anatomy of the Stomach
The mucosa of the stomach contains gastric glands and pyloric glands. The gastric glands respond to signals from the vagus nerve of the parasympathetic nervous system, which is activated by the brain in response to the sight, taste, and smell of food. Gastric glands have three different cell types: mucous cells, chief cells, and parietal cells. Mucous cells produce the bicarbonate-rich mucus that protects the muscular wall from the harshly acidic (pH = 2) and proteolytic environment of the stomach.
REAL WORLD
Nonsteroidal anti-inflammatory drugs (NSAIDs), such as ibuprofen, naproxen, and aspirin, are very common drugs. However, these drugs are not without side effects. One such side effect is the disruption of mucus production within the stomach. This leaves the mucosa of the stomach unprotected, and irritation results. This irritation can be in the form of gastritis, inflammation of the mucosa of the stomach, or gastric ulcers, deep wounds in the lining of the stomach.
Gastric juice is a combination of secretions from the other two cell types in the gastric glands: chief cells and parietal cells. The chief cells secrete pepsinogen. This is the inactive, zymogen form of pepsin, a proteolytic enzyme. Hydrogen ions in the stomach, secreted by parietal cells as hydrochloric acid, cleave pepsinogen to pepsin. Pepsin digests proteins by cleaving peptide bonds near aromatic amino acids, resulting in short peptide fragments. Because pepsin is activated by the acidic environment, it follows that pepsin is most active at a low pH. This is a unique characteristic among human enzymes, as most human enzymes are most active at physiological pH. Stomach acid also kills most harmful bacteria (with the exception of Helicobacter pylori, infection with which is usually asymptomatic but can cause inflammation, ulcers, and even certain gastric cancers). The acidic environment also helps to denature proteins and can break down some intramolecular bonds that hold food together. In addition to HCl, parietal cells secrete intrinsic factor, a glycoprotein involved in the proper absorption of vitamin B12.
KEY CONCEPT
The stomach secretes six products:
- HCl (kills microbes, denatures proteins, and converts pepsinogen into pepsin)
- Pepsinogen (cleaved in the stomach to pepsin; an enzyme that partially digests proteins)
- Mucus (protects mucosa)
- Bicarbonate (protects mucosa)
- Water (dissolves and dilutes ingested material)
- Intrinsic factor (required for normal absorption of vitamin B12)
The pyloric glands contain G-cells that secrete gastrin, a peptide hormone. Gastrin induces the parietal cells in the stomach to secrete more HCl and signals the stomach to contract, mixing its contents. The digestion of solid food in the stomach results in an acidic, semifluid mixture known as chyme. The combined mechanical and chemical digestive activities of the stomach result in a significant increase in the surface area of the now unrecognizable food particles, so when the chyme reaches the small intestine, the absorption of nutrients from it can be maximized. There are a few substances that are absorbed directly from the stomach (such as alcohol and aspirin), but the stomach is mainly an organ of digestion.
REAL WORLD
Zollinger–Ellison syndrome is a rare disease resulting from a gastrin-secreting tumor (gastrinoma). Typically, this tumor is found in the pancreas. The excess gastrin leads to excessive HCl production by parietal cells. Not surprisingly, one of the most common signs of Zollinger–Ellison syndrome is the presence of intractable ulcer disease.
Duodenum
The small intestine consists of three segments: the duodenum, the jejunum, and the ileum. The small intestine is quite long, up to seven meters. The duodenum is responsible for the majority of chemical digestion and has some minor involvement in absorption. However, most of the absorption in the small intestine takes place in the jejunum and ileum.
Food leaves the stomach through the pyloric sphincter and enters the duodenum. The presence of chyme in the duodenum causes the release of brush-border enzymes like disaccharidases (maltase, isomaltase, lactase, and sucrase) and peptidases (including dipeptidase). Brush-border enzymes are present on the luminal surface of cells lining the duodenum and break down dimers and trimers of biomolecules into absorbable monomers. The duodenum also secretes enteropeptidase, which is involved in the activation of other digestive enzymes from the accessory organs of digestion. Finally, it secretes hormones like secretin and cholecystokinin (CCK) into the bloodstream.
The disaccharidases digest disaccharides. Maltase digests maltose, isomaltase digests isomaltose, lactase digests lactose, and sucrase digests sucrose. Lack of a particular disaccharidase causes an inability to break down the corresponding disaccharide. Then bacteria in the intestines are able to hydrolyze that disaccharide, producing methane gas as a byproduct. In addition, undigested disaccharides can have an osmotic effect, pulling water into the stool and causing diarrhea. This is why people who are lactose intolerant have symptoms of bloating, flatulence, and possibly diarrhea after ingesting dairy products.
Peptidases break down proteins (or peptides, as the name implies). Aminopeptidase is a peptidase secreted by glands in the duodenum that removes the N-terminal amino acid from a peptide. Dipeptidases cleave the peptide bonds of dipeptides to release free amino acids. Unlike carbohydrates, which must be broken down into monosaccharides for absorption, proteins can be broken down into di- and even tripeptides and can be absorbed across the small intestine wall.
Enteropeptidase (formerly called enterokinase) is an enzyme critical for the activation of trypsinogen, a pancreatic protease, to trypsin. Trypsin then initiates an activation cascade, as described later in this chapter. Enteropeptidase can also activate procarboxypeptidases A and B to their active forms.
REAL WORLD
Celiac disease results from an immune reaction against gluten, a protein found in grains, especially wheat. In this condition, the immune system develops antibodies against certain components of gluten. These antibodies then cross-react with elements of the small intestine, causing damage to the mucosa. This results in diarrhea and discomfort. Sometimes, this condition also results in malabsorptive syndromes, including the inability to absorb fat and fat-soluble vitamins. Contrary to popular belief, celiac disease and gluten sensitivity are immune conditions, but not true allergies.
Secretin is a peptide hormone that causes pancreatic enzymes to be released into the duodenum. It also regulates the pH of the digestive tract by reducing HCl secretion from parietal cells and increasing bicarbonate secretion from the pancreas. Secretin is also an enterogastrone, a hormone that slows motility through the digestive tract. Slowing of motility allows increased time for digestive enzymes to act on chyme—especially fats.
Finally, cholecystokinin (CCK) is secreted in response to the entry of chyme (specifically, amino acids and fat in the chyme) into the duodenum. This peptide hormone stimulates the release of both bile and pancreatic juices and also acts in the brain, where it promotes satiety. Bile is a complex fluid composed of bile salts, pigments, and cholesterol. Bile salts are derived from cholesterol. They are not enzymes and therefore do not directly perform chemical digestion (the enzymatic cleavage of chemical bonds). However, bile salts serve an important role in the mechanical digestion of fats and ultimately facilitate the chemical digestion of lipids. Bile salts have hydrophobic and hydrophilic regions, allowing them to serve as a bridge between aqueous and lipid environments. In fact, bile salts are much like the common soaps and detergents we use to wash our hands, clothes, and dishes. In the small intestine, bile salts emulsify fats and cholesterol into micelles. Without bile, fats would spontaneously separate out of the aqueous mixture in the duodenum and would not be accessible to pancreatic lipase, which is water-soluble. In addition, these micelles increase the surface area of the fats, increasing the rate at which lipase can act. Ultimately, proper fat digestion depends on both bile and lipase. Bile gets the fats into the solution and increases their surface area by placing them in micelles (mechanical digestion). Then, lipase can come in to hydrolyze the ester bonds holding the lipids together (chemical digestion).
CCK also promotes the secretion of pancreatic juices into the duodenum, as shown in Figure 9.3. Pancreatic juices are a complex mixture of several enzymes in a bicarbonate-rich alkaline solution. This bicarbonate helps to neutralize acidic chyme, as well as provide an ideal working environment for the digestive enzymes, which are most active around pH 8.5. Pancreatic juices contain enzymes that can digest all three types of nutrients: carbohydrates, fats, and proteins. The identities and functions of these enzymes will be discussed in the next section of this chapter.
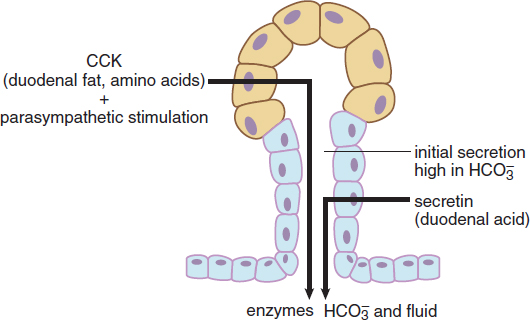
Figure 9.3. Hormonal Control of the Exocrine Pancreas
BRIDGE
The acidic environment of the stomach and basic environment of the duodenum point out the important correlation between pH and enzyme activity. Pepsin is active in the stomach and works best at pH 2. Pancreatic enzymes are active in the duodenum and work best at pH 8.5. pH, temperature, and salinity can all affect enzyme function, as highlighted in Chapter 2 of MCAT Biochemistry Review.
MCAT CONCEPT CHECK 9.2
Before you move on, assess your understanding of the material with these questions.
- What two main enzymes are found in saliva? What do these enzymes do?
-
-
- For each of the cell types below, list the major secretions of the cell and the functions of these secretions.
Cell Secretions Functions
Mucous cell Chief cell Parietal cell G-cell
- For each of the following substances, determine whether it is a digestive enzyme or a hormone and briefly summarize its functions.
Substance Enzyme or Hormone? Functions
Sucrase Secretin Dipeptidase Cholecystokinin Enteropeptidase
- How do bile and pancreatic lipase work together to digest fats?
9.3 Accessory Organs of Digestion
LEARNING OBJECTIVES
After Chapter 9.3, you will be able to:
- Recall the pancreatic enzymes and the molecules they help to digest
- Describe the significance and the function of bile, including its production, components, and release
- List the major functions of the liver
- Associate the accessory organs of digestion with their germ layer of origin
Digestion is a complex process that requires the release of enzymes not only from the cells directly lining the alimentary canal, but also from the pancreas, liver, and gallbladder. Collectively, these organs—which all originate as outgrowths of endoderm from the gut tube during development—are called accessory organs of digestion.
Pancreas
The pancreas serves two quite different roles in the body, reflecting its exocrine and endocrine functions. As discussed in Chapter 5 of MCAT Biology Review, the endocrine functions of the pancreas include the release of insulin, glucagon, and somatostatin—peptide hormones necessary for the maintenance of proper blood sugar levels. The hormonal function of the pancreas is limited to cells residing in islets of Langerhans scattered throughout the organ. The bulk of the pancreas, however, is made of exocrine cells called acinar cells that produce pancreatic juices. As mentioned earlier, pancreatic juices are bicarbonate-rich alkaline secretions containing many digestive enzymes that work on all three classes of biomolecules. Pancreatic amylase breaks down large polysaccharides into small disaccharides and is therefore responsible for carbohydrate digestion. The pancreatic peptidases (trypsinogen, chymotrypsinogen, and carboxypeptidases A and B) are released in their zymogen form, but once activated are responsible for protein digestion. Enteropeptidase, produced by the duodenum, is the master switch. It converts trypsinogen to trypsin, which can then activate the other zymogens, and also activates procarboxypeptidases A and B. Finally, the pancreas secretes pancreatic lipase, which is capable of breaking down fats into free fatty acids and glycerol.
Pancreatic juices are transferred to the duodenum via a duct system that runs along the middle of the pancreas, as shown in Figure 9.4. Like all exocrine cells, acinar cells secrete their products into ducts. These ducts then empty into the duodenum through the major and minor duodenal papillae.
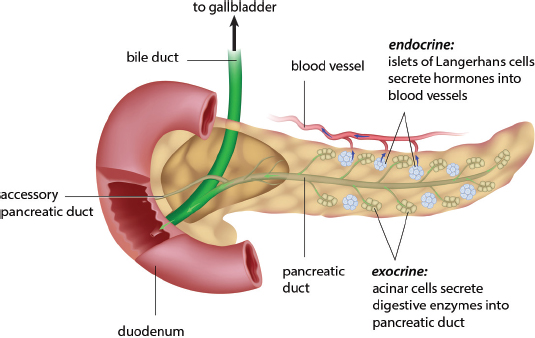
Figure 9.4. Anatomy of the Pancreas
REAL WORLD
Pancreatitis, or inflammation of the pancreas, is usually caused by gallstones or excessive consumption of alcohol. Regardless of the cause, pancreatitis results from premature activation of pancreatic enzymes and autodigestion of the pancreatic tissue. This is a very painful condition that may result in a long hospital stay and long-term consequences such as diabetes and the reduced digestion of proteins and fats.
Liver
The liver is located in the upper right quadrant of the abdomen and contains two unique structures for communicating with the digestive system. First, bile ducts connect the liver with both the gallbladder and small intestine. Bile is produced in the liver and travels down these bile ducts where it may be stored in the gallbladder or secreted into the duodenum. The liver also receives all blood draining from the abdominal portion of the digestive tract through the hepatic portal vein. This nutrient-rich blood can be processed by the liver before draining into the inferior vena cava on its way to the right side of the heart. For example, the liver takes up excess sugar to create glycogen, the storage form of glucose, and stores fats as triacylglycerols. The liver can also reverse these processes, producing glucose for the rest of the body through glycogenolysis and gluconeogenesis and mobilizing fats in lipoproteins. The liver detoxifies both endogenous compounds (those made in the body) and exogenous compounds (those brought in from the environment). For example, the liver converts ammonia, a toxic waste product of amino acid metabolism, into urea, which can be excreted by the kidneys. The liver also detoxifies and metabolizes alcohol and medications. Some drugs actually require activation by the enzymes of the liver. In addition, some drugs cannot be taken orally because modification of these drugs by the liver renders them inactive.
KEY CONCEPT
The functions of the liver include processing and synthesis of nutrients (glycogenesis and glycogenolysis, storage and mobilization of fats, gluconeogenesis), production of urea, detoxification of chemicals, production of bile, and synthesis of albumin and clotting factors.
Bile production is one of the most significant jobs of the liver vis-à-vis the digestive system. As mentioned earlier, bile is composed of bile salts, pigments, and cholesterol. Bile salts are amphipathic molecules that can emulsify fat in the digestive system. The major pigment in bile is bilirubin, which is a byproduct of the breakdown of hemoglobin. Bilirubin travels to the liver, where it is conjugated (attached to a protein) and secreted into the bile for excretion. If the liver is unable to process or excrete bilirubin (due to liver damage, excessive red blood cell destruction, or blockage of the bile ducts), jaundice or yellowing of the skin may occur.
KEY CONCEPT
The major components of bile are bile salts, which emulsify fats; pigments (especially bilirubin, from the breakdown of hemoglobin); and cholesterol.
In addition to bile production, processing of nutrients, and detoxification and drug metabolism, the liver also synthesizes certain proteins necessary for proper body function. These proteins include albumin, a protein that maintains plasma oncotic pressure and also serves as a carrier for many drugs and hormones, and clotting factors used during blood coagulation.
REAL WORLD
Cirrhosis of the liver can result from many different processes, including chronic alcohol consumption, hepatitis C infection, autoimmune hepatitis, and fatty liver disease. However, the outcome is the same. Cirrhosis is scarring of the liver, and this scar tissue builds up, creating increased resistance within the portal vein, resulting in portal hypertension. This causes a backup of fluid within the portal system, resulting in swollen veins in the digestive system, especially the esophagus, which may rupture and cause life-threatening bleeding. This often manifests as hematemesis, or vomiting of blood. Cirrhosis also causes bleeding disorders because production of clotting factors is disrupted. The inability to properly dispose of ammonia results in increased ammonia in the blood, which affects mentation. Finally, cirrhosis may also cause hepatocellular carcinoma, or cancer of the hepatocytes.
Gallbladder
The gallbladder is located just beneath the liver and both stores and concentrates bile. Upon release of CCK, the gallbladder contracts and pushes bile out into the biliary tree. The bile duct system merges with the pancreatic duct, as shown in Figure 9.4 earlier, before emptying into the duodenum.
The gallbladder is a common site of cholesterol or bilirubin stone formation. This painful condition causes inflammation of the gallbladder. The stones may also travel into the bile ducts and get stuck in the biliary tree. In some cases, stones can get caught just before entering the duodenum, resulting in blockage of not only the biliary tree, but the pancreatic duct as well, causing pancreatitis.
BRIDGE
Stone formation is nothing more than precipitation of a solid once its concentration has reached the Ksp of the compound. This is particularly common in the gallbladder because bile is concentrated there. Solubility and Ksp are discussed in Chapter 9 of MCAT General Chemistry Review.
The functions of the various digestive enzymes (and bile) are summarized in Table 9.1.
Table 9.1. Digestive Enzymes
NUTRIENT ENZYME SITE OF PRODUCTION SITE OF FUNCTION FUNCTION
Carbohydrates
Salivary amylase (ptyalin) Salivary glands Mouth Hydrolyzes starch to maltose and dextrins
Pancreatic amylase Pancreas (acinar cells) Duodenum Hydrolyzes starch to maltose and dextrins
Maltase Intestinal glands Duodenum Hydrolyzes maltose to two glucose molecules
Isomaltase Intestinal glands Duodenum Hydrolyzes isomaltose to two glucose molecules
Sucrase Intestinal glands Duodenum Hydrolyzes sucrose to glucose and fructose
Lactase Intestinal glands Duodenum Hydrolyzes lactose to glucose and galactose
Proteins
Pepsin(ogen) Gastric glands (chief cells) Stomach Hydrolyzes specific peptide bonds; activated by HCl
Trypsin(ogen) Pancreas (acinar cells) Duodenum Hydrolyzes specific peptide bonds; converts chymotrypsinogen to chymotrypsin; activated by enteropeptidase
Chymotrypsin (ogen) Pancreas (acinar cells) Duodenum Hydrolyzes specific peptide bonds; activated by trypsin
(Pro)carboxy peptidases A and B Pancreas (acinar cells) Duodenum Hydrolyzes terminal peptide bond at carboxy end; activated by enteropeptidase
Aminopeptidase Intestinal glands Duodenum Hydrolyzes terminal peptide bond at amino end
Dipeptidases Intestinal glands Duodenum Hydrolyzes pairs of amino acids
Enteropeptidase Intestinal glands Duodenum Converts trypsinogen to trypsin and procarboxypeptidases A and B to carboxypeptidases A and B
Lipids
Bile* Liver (stored in gallbladder) Duodenum Emulsifies fat
Lipase Pancreas (acinar cells) Duodenum Hydrolyzes lipids
*Note: Bile is not an enzyme, but is involved in mechanical digestion of fats.
A summary of the digestion of each major class of biomolecules is provided in Figure 9.5.
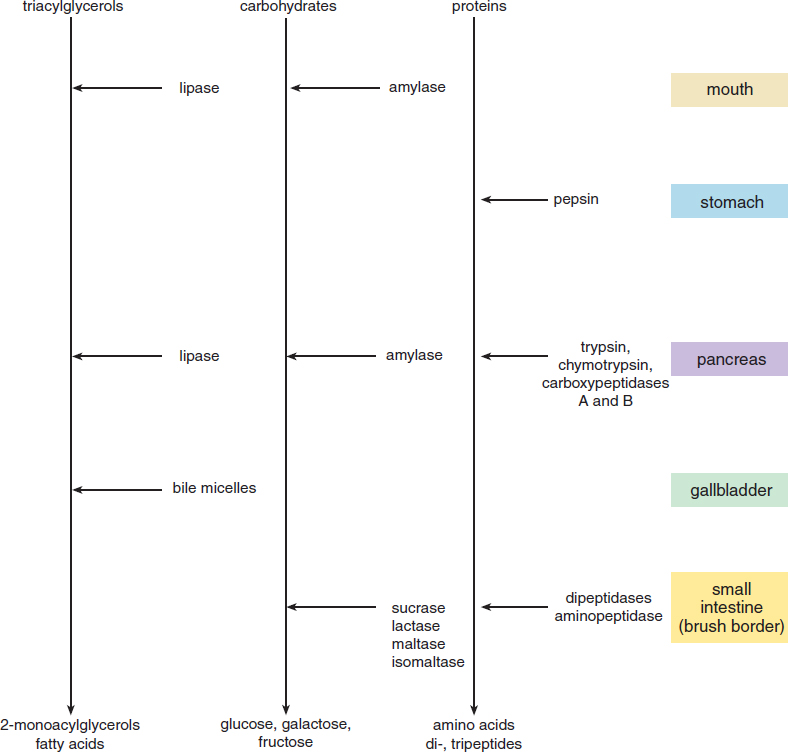
Figure 9.5. Summary of Digestive Processes
MCAT CONCEPT CHECK 9.3
Before you move on, assess your understanding of the material with these questions.
- List at least one pancreatic enzyme that digests each of the three major classes of biomolecules:
- Carbohydrates:
- Proteins:
- Fats:
- What are the main components of bile?
- Where is bile synthesized? Where is bile stored? Where does bile carry out its digestive function?
- Synthesized:
- Stored:
- Carries out function:
- List at least four functions of the liver:
-
-
-
-
- The accessory organs of digestion originate from which primary germ layer?
9.4 Absorption and Defecation
LEARNING OBJECTIVES
After Chapter 9.4, you will be able to:
- Recall the four fat-soluble vitamins
- Order the three sections of the small intestine and the three sections of the large intestine
- Predict the portions of the gut impacted by a disease when given a digestive symptom, such as watery stool
- Identify the biomolecules typically absorbed into each vessel of the villus:
Absorption of nutrients primarily occurs in the small intestine, especially in the jejunum and ileum. The large intestine largely absorbs water.
Jejunum and Ileum
The small intestine consists of three segments: the duodenum, the jejunum, and the ileum. As discussed previously, the duodenum is primarily involved in digestion. The jejunum and ileum are involved in the absorption of nutrients. The small intestine is lined with villi, which are small, finger-like projections from the epithelial lining, as shown in Figure 9.6. Each villus has many microvilli, drastically increasing the surface area available for absorption. In addition, at the middle of each villus there is a capillary bed for the absorption of water-soluble nutrients and a lacteal, a lymphatic channel that takes up fats for transport into the lymphatic system.
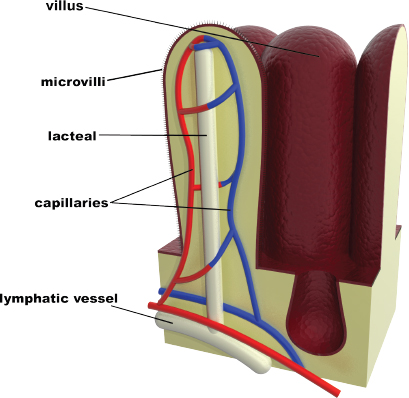
Figure 9.6. Structure of a Villus
MNEMONIC
Segments of the small intestine: Dow Jones Industrial
- Duodenum
- Jejunum
- Ileum
Simple sugars, such as glucose, fructose, and galactose, and amino acids are absorbed by secondary active transport and facilitated diffusion into the epithelial cells lining the small intestine, as shown in Figure 9.7. Then, these substances move across the epithelial cell membrane into the intestinal capillaries. Blood is constantly passing by the epithelial cells, carrying the carbohydrate and amino acid molecules away. This creates a concentration gradient such that the blood always has a lower concentration of monosaccharides and amino acids than inside the epithelial cells. Thus, simple carbohydrates and amino acids diffuse from the epithelial cells into the capillaries. The absorbed molecules then go to the liver via the hepatic portal circulation.
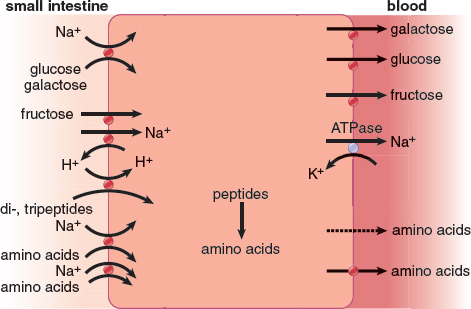
Figure 9.7. Absorption of Carbohydrates and Amino Acids in the Small Intestine
What about fats? Short-chain fatty acids will follow the same process as carbohydrates and amino acids by diffusing directly into the intestinal capillaries. These fatty acids do not require transporters because they are nonpolar, so they can easily traverse the cellular membrane. Larger fats, glycerol, and cholesterol move separately into the intestinal cells but then reform into triglycerides, as shown in Figure 9.8. The triglycerides and esterified cholesterol molecules are packaged into chylomicrons. Rather than entering the bloodstream, chylomicrons enter the lymphatic circulation through lacteals, small vessels that form the beginning of the lymphatic system. These lacteals converge and enter the venous circulation at the thoracic duct in the base of the neck, which empties into the left subclavian vein.
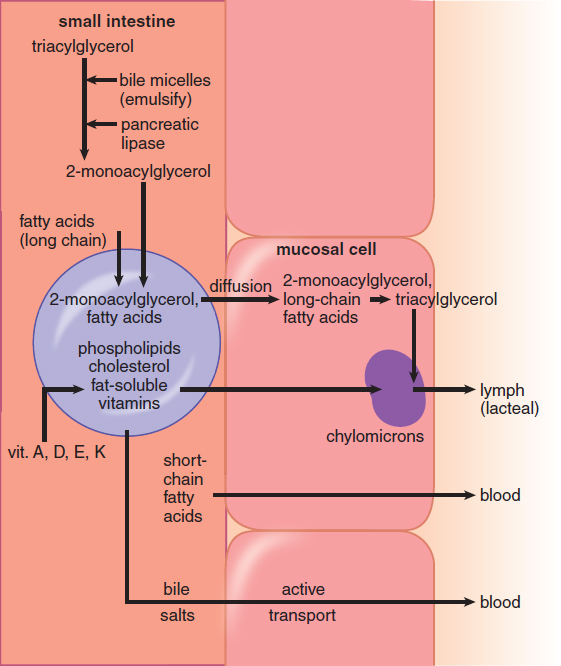
Figure 9.8. Absorption of Lipids
Vitamins are also absorbed in the small intestine. Vitamins can be categorized as either fat-soluble or water-soluble. Because there are only four fat-soluble vitamins (A, D, E, and K), these can be easily memorized. All other vitamins (B complex and C) are water-soluble. Fat-soluble vitamins dissolve directly into chylomicrons to enter the lymphatic circulation. Failure to digest and absorb fat properly, which can be due to pathologies in the liver, gallbladder, pancreas, or small intestine, may lead to deficiencies of fat-soluble vitamins. The water-soluble vitamins are taken up, along with water, amino acids, and carbohydrates, across the endothelial cells of the small intestine, passing directly into the plasma.
In addition to fats, carbohydrates, amino acids, and vitamins, the small intestine also absorbs water. Much of the water in chyme is actually the result of secretions. On average, a person may consume up to two liters of fluid per day, but secretions into the upper gastrointestinal tract may total up to seven liters of fluid per day. In order to maintain proper fluid levels within the body, much of this fluid must be reabsorbed by osmosis. As solutes are absorbed into the bloodstream, water is drawn with them, eventually reaching the capillaries. Water passes not only transcellularly (across the cell membrane), but also paracellularly (squeezing between cells) to reach the blood.
Large Intestine
The final part of the gastrointestinal tract is the large intestine. It is primarily involved in water absorption. The large intestine has a larger diameter but shorter length than the small intestine. It is divided into three major sections: the cecum, the colon, and the rectum. The cecum is simply an outpocketing that accepts fluid exiting the small intestine through the ileocecal valve and is the site of attachment of the appendix. The appendix is a small finger-like projection that was once thought to be vestigial. Recent evidence, however, suggests that it may have a role in warding off certain bacterial infections and repopulating the large intestine with normal flora after episodes of diarrhea. Inflammation of the appendix (appendicitis) is a surgical emergency; in fact, it is the most common reason for an unscheduled surgery in the United States.
The colon itself is divided into the ascending, transverse, descending, and sigmoid colons. Its main function is to absorb water and salts (such as sodium chloride) from the undigested material left over from the small intestine. The small intestine actually absorbs much more water than the colon, so the colon primarily concentrates the remaining material to form feces. Too little or too much water absorption can cause diarrhea or constipation, respectively.
BRIDGE
Note the similarity between the muscles that control voiding of urine and feces. In both cases, there is an internal sphincter under autonomic control (internal urethral sphincter and internal anal sphincter) and an external sphincter under somatic control (external urethral sphincter and external anal sphincter). Urination is discussed in Chapter 10 of MCAT Biology Review.
Finally, the rectum serves as a storage site for feces, which consists of indigestible material, water, bacteria (E. coli and others), and certain digestive secretions that are not reabsorbed (enzymes and some bile). The anus is the opening through which wastes are eliminated and consists of two sphincters: the internal and external anal sphincters. The external sphincter is under voluntary control (somatic), but the internal sphincter is under involuntary control (autonomic).
The large intestine—and even the small intestine—is home to many different species of bacteria. In fact, 30 percent of the dry matter in stool consists of bacteria. Most of these bacteria are anaerobes, but the cecum is also home to many aerobic bacteria. The presence of bacteria in the colon represents a symbiotic relationship: the bacteria are provided with a steady source of food, and the byproducts produced by the bacteria are beneficial to humans. For example, bacteria in the gut produce vitamin K, which is essential for the production of clotting factors, and biotin (vitamin B7), which is a coenzyme for many metabolic enzymes.
MCAT CONCEPT CHECK 9.4
Before you move on, assess your understanding of the material with these questions.
- What are the two circulatory vessels in a villus? What biomolecules are absorbed into each?
-
-
- What are the four fat-soluble vitamins?
- What are the three sections of the small intestine, in order? What are the three sections of the large intestine, in order?
- Small intestine: ________,______,________
- Large intestine: ________,______,________
- Vibrio cholera causes a severe infection in the intestines, leading to massive volumes of watery diarrhea—up to 20 liters per day. Given these symptoms, does cholera likely impact the small intestine or the large intestine?
Conclusion
In this chapter, we have reviewed a lot of information about the digestive system that we can use to our advantage on Test Day. We began with an overview of the anatomy, keeping in mind that the system is designed to carry out extracellular digestion. Considering that all our foodstuffs are made up of fats, proteins, and carbohydrates, these compounds have to be broken down to their simplest molecular forms before they can be absorbed and distributed to the tissues and cells of the body. As we moved through the gastrointestinal tract, we discussed whether each organ was a site of absorption, digestion, or both. We spent a good bit of time discussing each of the enzymes involved in digestion and their specific purposes. While digestion occurs primarily in the oral cavity, stomach, and duodenum, absorption occurs primarily in the jejunum and ileum, where the method of transport into the circulatory system is slightly different depending on the compound. Finally, we discussed the three segments of the large intestine and their roles in water and salt absorption, as well as the temporary storage of waste products. Although the amount of information about the digestive system may seem overwhelming, the underlying concepts are relatively straightforward, and a systematic approach (such as charts, tables, or flashcards) will help you manage this content.
In the end, the digestive system’s main purpose is to break down energy-containing compounds and get them into the circulation so they can be used by the rest of the body. Equally important are the systems the body has for getting rid of compounds from the blood. Buildup of waste products like ammonia, urea, potassium, and hydrogen ions can lead to serious pathology. For instance, hyperammonemia (buildup of ammonia in the blood) can lead to severe, permanent neurological damage. Hyperkalemia (buildup of potassium in the blood) can quickly cause a fatal heart attack. Temperature regulation is similarly important; both hyperthermia and hypothermia can lead to organ dysfunction and, ultimately, death. In the next chapter, we turn our attention to these regulatory systems: the renal system and the skin.
GO ONLINE
You've reviewed the content, now test your knowledge and critical thinking skills by completing a test-like passage set in your online resources!
CONCEPT SUMMARY
Anatomy of the Digestive System
- Intracellular digestion involves the oxidation of glucose and fatty acids to make energy. Extracellular digestion occurs in the lumen of the alimentary canal.
- Mechanical digestion is the physical breakdown of large food particles into smaller food particles.
- Chemical digestion is the enzymatic cleavage of chemical bonds, such as the peptide bonds of proteins or the glycosidic bonds of starches.
- The pathway of the digestive tract is: oral cavity → pharynx → esophagus → stomach → small intestine → large intestine → rectum
- The accessory organs of digestion are the salivary glands, pancreas, liver, and gallbladder.
- The enteric nervous system is in the wall of the alimentary canal and controls peristalsis. Its activity is upregulated by the parasympathetic nervous system and downregulated by the sympathetic nervous system.
Ingestion and Digestion
- Multiple hormones regulate feeding behavior, including antidiuretic hormone (ADH or vasopressin) and aldosterone, which promote thirst; glucagon and ghrelin, which promote hunger; and leptin and cholecystokinin, which promote satiety.
- In the oral cavity, mastication starts the mechanical digestion of food, while salivary amylase and lipase start the chemical digestion of food. Food is formed into a bolus and swallowed.
- The pharynx connects the mouth and posterior nasal cavity to the esophagus.
- The esophagus propels food to the stomach using peristalsis. Food enters the stomach through the lower esophageal (cardiac) sphincter.
- The stomach has four parts: fundus, body, antrum, and pylorus. The stomach has a lesser and greater curvature and is thrown into folds called rugae. Numerous secretory cells line the stomach.
- Mucous cells produce bicarbonate-rich mucus to protect the stomach.
- Chief cells secrete pepsinogen, a protease activated by the acidic environment of the stomach.
- Parietal cells secrete hydrochloric acid and intrinsic factor, which is needed for vitamin B12 absorption.
- G-cells secrete gastrin, a peptide hormone that increases HCl secretion and gastric motility.
- After mechanical and chemical digestion in the stomach, the food particles are now called chyme. Food passes into the duodenum through the pyloric sphincter.
- The duodenum is the first part of the small intestine and is primarily involved in chemical digestion.
- Disaccharidases are brush-border enzymes that break down maltose, isomaltose, lactose, and sucrose into monosaccharides.
- Brush-border peptidases include aminopeptidase and dipeptidases.
- Enteropeptidase activates trypsinogen and procarboxypeptidases, initiating an activation cascade.
- Secretin stimulates the release of pancreatic juices into the digestive tract and slows motility.
- Cholecystokinin stimulates bile release from the gallbladder, release of pancreatic juices, and satiety.
Accessory Organs of Digestion
- Acinar cells in the pancreas produce pancreatic juices that contain bicarbonate, pancreatic amylase, pancreatic peptidases (trypsinogen, chymotrypsinogen, carboxypeptidases A and B), and pancreatic lipase.
- The liver synthesizes bile, which can be stored in the gallbladder or secreted into the duodenum directly.
- Bile emulsifies fats, making them soluble and increasing their surface area.
- The main components of bile are bile salts, pigments (especially bilirubin from the breakdown of hemoglobin), and cholesterol.
- The liver also processes nutrients (through glycogenesis and glycogenolysis, storage and mobilization of fats, and gluconeogenesis), produces urea, detoxifies chemicals, activates or inactivates medications, produces bile, and synthesizes albumin and clotting factors.
- The gallbladder stores and concentrates bile.
Absorption and Defecation
- The jejunum and ileum of the small intestine are primarily involved in absorption.
- The small intestine is lined with villi, which are covered with microvilli, increasing the surface area available for absorption.
- Villi contain a capillary bed and a lacteal, a vessel of the lymphatic system.
- Water-soluble compounds, such as monosaccharides, amino acids, water-soluble vitamins, small fatty acids, and water, enter the capillary bed.
- Fat-soluble compounds, such as fats, cholesterol, and fat-soluble vitamins, enter the lacteal.
- The large intestine absorbs water and salts, forming semisolid feces.
- The cecum is an outpocketing that accepts fluid from the small intestine through the ileocecal valve and is the site of attachment of the appendix.
- The colon is divided into ascending, transverse, descending, and sigmoid portions.
- The rectum stores feces, which are then excreted through the anus.
- Gut bacteria produce vitamin K and biotin (vitamin B7).
ANSWERS TO CONCEPT CHECKS
**9.1**
- Mechanical digestion, such as chewing, physically breaks down food into smaller pieces. Chemical digestion involves hydrolysis of bonds and breakdown of food into smaller biomolecules.
- Oral cavity (mouth) → pharynx → esophagus → stomach → small intestine → large intestine → rectum → anus
- The parasympathetic nervous system increases secretions from all of the glands of the digestive system and promotes peristalsis. The sympathetic nervous system slows peristalsis.
**9.2**
- Saliva contains salivary amylase (ptyalin), which digests starch into smaller sugars (maltose and dextrin); and lipase, which digests fats.
-
Cell Secretions Functions
Mucous cell Mucus Protects lining of stomach, increases pH (bicarbonate)
Chief cell Pepsinogen Digests proteins, activated by H+
Parietal cell HCl, intrinsic factor HCl: decreases pH, kills microbes, denatures proteins, carries out some chemical digestion; intrinsic factor: absorption of vitamin B12
G-cell Gastrin Increases HCl production, increases gastric motility
-
Substance Enzyme or Hormone? Functions
Sucrase Enzyme Brush-border enzyme; breaks down sucrose into monosaccharides
Secretin Hormone Increases pancreatic secretions, especially bicarbonate; reduces HCl secretion; decreases motility
Dipeptidase Enzyme Brush-border enzyme; breaks down dipeptides into free amino acids
Cholecystokinin Hormone Recruits secretions from gallbladder and pancreas; promotes satiety
Enteropeptidase Enzyme Activates trypsinogen, which initiates an activation cascade
- Bile accomplishes mechanical digestion of fats, emulsifying them and increasing their surface area. Pancreatic lipase accomplishes chemical digestion of fats, breaking their ester bonds.
**9.3**
- Carbohydrates: pancreatic amylase; proteins: trypsin, chymotrypsin, carboxypeptidases A and B; fats: pancreatic lipase
- Bile is composed of bile salts (amphipathic molecules derived from cholesterol that emulsify fats), pigments (especially bilirubin from the breakdown of hemoglobin), and cholesterol.
- Bile is synthesized in the liver, stored in the gallbladder, and serves its function in the duodenum.
- The liver processes nutrients (through glycogenesis and glycogenolysis, storage and mobilization of fats, and gluconeogenesis), produces urea, detoxifies chemicals, activates or inactivates medications, produces bile, and synthesizes albumin and clotting factors.
- As outgrowths of the gut tube, the accessory organs of digestion arise from embryonic endoderm.
**9.4**
- The two circulatory vessels are capillaries and lacteals. The capillary absorbs water-soluble nutrients like monosaccharides, amino acids, short-chain fatty acids, water-soluble vitamins, and water itself. The lacteal absorbs fat-soluble nutrients, like fats, cholesterol, and fat-soluble vitamins.
- The fat-soluble vitamins are A, D, E, and K.
- The small intestine consists of the duodenum, jejunum, and ileum. The large intestine consists of the cecum, colon, and rectum.
- While the large intestine’s main function is to absorb water, the small intestine actually absorbs a much larger volume of water. Thus, massive volumes of watery diarrhea are more likely to arise from infections in the small intestine than in the large intestine.
SCIENCE MASTERY ASSESSMENT EXPLANATIONS
1. B
Chief cells secrete pepsinogen, a protease secreted as a zymogen that is activated by the acidic environment of the stomach. G-cells secrete gastrin, parietal cells secrete hydrochloric acid and intrinsic factor, and mucous cells secrete alkaline mucus, eliminating the other answer choices.
2. B
The small intestine is divided into three sections: the duodenum, the jejunum, and the ileum. The cecum is part of the large intestine, making (B) the correct answer.
3. B
Aminopeptidase is a brush-border peptidase secreted by the cells lining the duodenum; it does not require enteropeptidase for activation. Both trypsinogen and procarboxypeptidases A and B are activated by enteropeptidase, eliminating (A) and (D). Once activated, trypsin can activate chymotrypsinogen; if trypsinogen cannot be activated, then chymotrypsinogen will not be activated either, eliminating (C).
4. D
Lipase is involved in the digestion of fats, but its function is not to emulsify fats—this is the job of bile. Rather, lipase chemically digests fats in the duodenum, allowing them to be brought into duodenal cells and packaged into chylomicrons. The other associations given here are all correct.
5. C
Protein digestion begins in the stomach, where pepsin (secreted as pepsinogen) hydrolyzes specific peptide bonds. Protein digestion continues in the small intestine as trypsin (secreted as trypsinogen), chymotrypsin (secreted as chymotrypsinogen), carboxypeptidases A and B (secreted as procarboxypeptidases A and B), aminopeptidase, and dipeptidases hydrolyze specific parts of the peptide. No protein digestion occurs in the mouth or large intestine.
6. A
Sucrase is a brush-border enzyme found on duodenal cells and is not secreted by the salivary glands. This enzyme hydrolyzes sucrose (a disaccharide) to form glucose and fructose (monosaccharides). The other associations are all correct.
7. B
The question is basically asking us to identify the structure that lies between the stomach and the small intestine. This is the pyloric sphincter; the presentation given in the question is a classic example of what is called pyloric stenosis, in which the pyloric sphincter is thickened and cannot relax to permit chyme through. The cardiac sphincter, (A), lies between the esophagus and the stomach. The ileocecal valve, (C), lies between the ileum of the small intestine and the cecum of the large intestine. The internal anal sphincter, (D), lies at the end of the rectum.
8. B
The parasympathetic nervous system has many roles in the digestive system. It promotes motility of the gut tube and secretion from glands. Therefore, blocking the parasympathetic nervous system would likely result in dry mouth (from reduced secretion of saliva), slow gastric emptying (from decreased peristalsis), and decreased gastric acid production (from reduced HCl secretion from the parietal cells in the gastric glands), eliminating (A), (C), and (D). (B) is the correct answer because we would expect constipation in such an individual, not diarrhea: slowed motility through the colon would lead to increased water reabsorption, making the feces too firm and causing constipation.
9. B
The first graph shows maximal activity at a very acidic pH, implying that this is an enzyme acting in the stomach. The second graph shows maximal activity around pH 8.5, implying that this is an enzyme acting in the duodenum. The only choice that matches the first graph with a stomach enzyme (pepsin) and the second with a duodenal enzyme (carboxypeptidase B) is (B).
10. C
Elevated bilirubin implies a blockage to bile flow, increased production of bilirubin (from massive hemoglobin release), or an inability of the liver to produce bile. If the bile duct were occluded, as in (A), then bile would not be able to flow into the digestive tract and would build up, increasing bilirubin levels in the blood. If many red blood cells were lysed, as in (B), then bilirubin levels would rise in accordance with the increased hemoglobin release. If liver failure occurred, as in (D), then the liver would be unable to produce bile, and bilirubin would again build up. (C) refers to a pathology in the stomach—the key word given here is rugae, which are the folds in the stomach wall. Lack of gastric function would have no effect on bilirubin levels, making this the correct choice.
11. A
Chylomicrons contain triacylglycerols, cholesteryl esters, and fat-soluble vitamins and are secreted by intestinal cells into lacteals. Amino acids, fat-soluble vitamins (like vitamins A and E), and cholesterol are all absorbed in the small intestine.
12. B
The cleavage of a fat described in this question stem refers to the breakdown of triacylglycerides, which is a hydrolysis reaction in which water is added across the ester linkage of the fatty acids to the glycerol backbone, breaking these bonds. For this reason, chemical digestion, (B), is correct. Note that, the location of this reaction occurs in the lumen of a digestive organ, so this reaction could also be classified as an extracellular reaction. This observation is important because it eliminates (C).
13. A
While the capillaries from the intestine come together to form the portal vein, which drains to the liver, the lacteals come together to form the thoracic duct, which drains directly into the left subclavian vein. Therefore, fat-soluble compounds do not pass through the liver before reaching the right side of the heart. Only (A), vitamin D, is fat-soluble.
14. C
Ghrelin promotes a sensation of hunger, increasing feeding behavior. Both leptin and cholecystokinin promote satiety, decreasing feeding behavior—eliminating (A) and (B). Gastrin increases acid production and gastric motility, but does not have any significant relationship with feeding behavior, eliminating (D).
15. D
The liver serves many functions, including carrying out metabolic processes (glycogenesis and glycogenolysis, fat storage, and gluconeogenesis), detoxification or activation of medications, and synthesis of bile. Germane to this question are the roles of converting ammonia into urea through the urea cycle and synthesis of proteins, including albumin and clotting factors. A patient with liver failure would thus not be able to convert ammonia into urea and would have high concentrations of ammonia and low concentrations of urea in the blood, eliminating (A) and (C). With decreased synthetic activity, both albumin and clotting factor concentrations would be low, eliminating (B) and making (D) the correct answer.
GO ONLINE
Consult your online resources for additional practice.
SHARED CONCEPTS
Biochemistry Chapter 2
Enzymes
Biochemistry Chapter 9
Carbohydrate Metabolism I
Biochemistry Chapter 11
Lipid and Amino Acid Metabolism
Biology Chapter 5
The Endocrine System
Biology Chapter 7
The Cardiovascular System
Biology Chapter 8
The Immune System