Chapter 11: The Musculoskeletal System
Chapter 11: The Musculoskeletal System
SCIENCE MASTERY ASSESSMENT
Every pre-med knows this feeling: there is so much content I have to know for the MCAT! How do I know what to do first or what's important?
While the high-yield badges throughout this book will help you identify the most important topics, this Science Mastery Assessment is another tool in your MCAT prep arsenal. This quiz (which can also be taken in your online resources) and the guidance below will help ensure that you are spending the appropriate amount of time on this chapter based on your personal strengths and weaknesses. Don't worry though— skipping something now does not mean you'll never study it. Later on in your prep, as you complete full-length tests, you'll uncover specific pieces of content that you need to review and can come back to these chapters as appropriate.
How to Use This Assessment
If you answer 0–7 questions correctly:
Spend about 1 hour to read this chapter in full and take limited notes throughout. Follow up by reviewing all quiz questions to ensure that you now understand how to solve each one.
If you answer 8–11 questions correctly:
Spend 20–40 minutes reviewing the quiz questions. Beginning with the questions you missed, read and take notes on the corresponding subchapters. For questions you answered correctly, ensure your thinking matches that of the explanation and you understand why each choice was correct or incorrect.
If you answer 12–15 questions correctly:
Spend less than 20 minutes reviewing all questions from the quiz. If you missed any, then include a quick read-through of the corresponding subchapters, or even just the relevant content within a subchapter, as part of your question review. For questions you answered correctly, ensure your thinking matches that of the explanation and review the Concept Summary at the end of the chapter.
Questions 1, 2, and 3 are based on the following diagram:
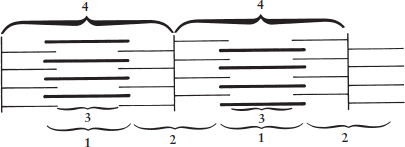
- During muscle contraction, which of the following regions decrease(s) in length?
- 1 only
- 1 and 2 only
- 3 and 4 only
- 2, 3, and 4 only
- Region 1 refers to:
- the thick filaments only.
- the thin filaments only.
- the A-band.
- the I-band.
- Which region represents one sarcomere?
- 1
- 2
- 3
- 4
- With which of the following molecules does Ca2+ bind after its release from the sarcoplasmic reticulum to regulate muscle contraction?
- Myosin
- Actin
- Troponin
- Tropomyosin
- Which of the following cells is correctly coupled with its definition?
- Osteoblasts—bone cells involved in the secretion of bone matrix
- Osteoclasts—immature bone cells
- Osteocytes—polynucleated cells actively involved in bone resorption
- Chondrocytes—undifferentiated bone marrow cells
- An X-ray of the right femur in a child shows that it is shorter than the opposite femur, and below the average length for a child of this age. Which region of the bone is most likely to have caused this abnormality?
- Diaphysis
- Metaphysis
- Epiphysis
- Periosteum
- Which of the following INCORRECTLY pairs a type of muscle fiber with a characteristic of that fiber?
- Red fibers—rich in mitochondria
- Red fibers—high levels of myoglobin
- White fibers—fast-twitching
- White fibers—predominantly use aerobic respiration
- When the knee moves back and forth during walking, what prevents the surfaces of the leg bones from rubbing against each other?
- Articular cartilage
- Epiphyses
- Synovial fluid
- Smooth muscle
- Which type(s) of muscle is/are always multinucleated?
- Cardiac muscle
- Skeletal muscle
- Smooth muscle
- I only
- II only
- III only
- I and II only
- Which type(s) of muscle has/have myogenic activity?
- Cardiac muscle
- Skeletal muscle
- Smooth muscle
- I only
- II only
- III only
- I and III only
- Red bone marrow is involved in erythrocyte formation. In contrast, yellow bone marrow:
- is involved in leukocyte formation.
- is responsible for drainage of lymph.
- causes the formation of spicules.
- contains predominantly adipose tissue.
- Which of the following statements regarding the periosteum is INCORRECT?
- The periosteum serves as a site of attachment of bone to muscle.
- Cells of the periosteum may differentiate into osteoblasts.
- The periosteum is a fibrous sheath that surrounds long bones.
- The periosteum secretes fluid into the joint cavity.
- Which of the following bones is NOT a part of the appendicular skeleton?
- The triquetrum, one of the carpal bones
- The calcaneus, which forms the heel
- The ischium, one of the fused pelvic bones
- The sternum, or breastbone
- To facilitate the process of birth, an infant’s head is somewhat flexible. This flexibility is due in part to the two fontanelles, which are soft spots of connective tissue in the infant’s skull. With time, the fontanelles will close through a process known as:
- endochondral ossification.
- intramembranous ossification.
- bone resorption.
- longitudinal growth.
- A young patient presents to the emergency room with a broken hip. The patient denies any recent history of trauma to the joint. Blood tests reveal a calcium concentration of 11.5 mg dL (normal: 8.4–10.2). Which tissue is likely responsible for these findings?
- Thyroid
- Cartilage
- Parathyroid
- Smooth muscle
Answer Key
- D
- C
- D
- C
- A
- C
- D
- A
- B
- D
- D
- D
- D
- B
- C
Chapter 11: The Musculoskeletal System
CHAPTER 11
THE MUSCULOSKELETAL SYSTEM
In This Chapter
11.1 The Muscular System
Types of Muscle
Microscopic Structure of Skeletal Muscle
Muscle Contraction
Stimulation, Summation, and Muscle Fatigue
11.2 The Skeletal System
Skeletal Structure
Bone Composition
Cartilage
Joints and Movement
Concept Summary
CHAPTER PROFILE
The content in this chapter should be relevant to about 8% of all questions about biology on the MCAT.
This chapter covers material from the following AAMC content category:
3B: Structure and integrative functions of the main organ systems
Introduction
Large disasters or traumatic events like wars or earthquakes can deeply affect the health of populations, which also has an impact on the practice of medicine, sometimes leading to the discovery of new medical conditions. During World War II, Nazi Germany bombed London for 57 consecutive days during the beginning of what came to be known as the Blitzkrieg, or an eight-month “lightning war.” Victims of the Blitz, as it is known in London, included those afflicted with a specific set of symptoms: pain and swelling with accompanying effects of depleted blood volume (shock, weakness, low blood pressure, and decreased urine output). Less obvious was acute kidney failure, which could lead quickly to death if left untreated.
What caused the Blitz victims to suffer from these symptoms? Extreme physical trauma to muscles—namely, compression—destroys skeletal muscle tissue. This condition is called rhabdomyolysis (rhabdo– refers to striation, myo– to muscle, and –lysis to breakdown). The products of skeletal muscle destruction, some of which are toxic, circulate in the blood until they are filtered out. Creatine kinase is one of these products; in fact, rhabdomyolysis is diagnosed with a creatine kinase level five times the normal upper limit. Myoglobin is another. Much like hemoglobin, myoglobin uses heme to carry oxygen; it is not, however, housed within a red blood cell. Thus, an erythrocyte-free urine sample that tests positive for heme points compellingly toward rhabdomyolysis. Myoglobin oxygen reserves are just one of the specialized features of muscles, as we will see in this chapter.
Skeletal muscles are only able to exert an effect on the body by moving bony structures around joints. Further, skeletal muscle isn’t the only form of muscle in the body; smooth muscle plays roles in the cardiovascular, respiratory, reproductive, and digestive systems, and cardiac muscle comprises the contractile tissue of the heart. Bones are more than simply a support structure, however; they also provide protection to internal organs, serve as a storage reserve of calcium and other minerals, and are the site of hematopoiesis. In this chapter, we’ll explore the biology of all of these tissues, completing our tour of systems anatomy and physiology.
11.1 The Muscular System
LEARNING OBJECTIVES
After Chapter 11.1, you will be able to:
- Categorize muscles as skeletal, smooth, or cardiac based on their innervation and structure
- Order the series of events in muscular contraction
- Explain the relationship between ATP binding and muscular contraction
- Recall the meaning of the terms summation, simple twitch, and tetanus
- Identify the zones and bands within a sarcomere and predict their length changes during contraction:

The muscular system is composed of not only skeletal muscle, but also smooth muscle and cardiac muscle. Skeletal muscle is essential for supporting the body and facilitating movement. The contraction of skeletal muscle also compresses venous structures and helps propel blood through the low-pressure venous system toward the heart, as well as lymph through the lymphatic system. Rapid muscle contraction also leads to shivering, which is important in thermoregulation. Smooth muscle is responsible for involuntary movement, such as the rhythmic contractions of smooth muscle in the digestive system called peristalsis. Smooth muscle also aids in the regulation of blood pressure by constricting and relaxing the vasculature. Cardiac muscle is a special type of muscle that is able to maintain rhythmic contraction of the heart without nervous system input. In this section, we will discuss each type of muscle as well as the physiology of muscles.
Types of Muscle
Muscle can be divided into the three different subtypes: skeletal muscle, smooth muscle, and cardiac muscle. Each muscle type performs specific functions, although they share some similarities. All muscle is capable of contraction, which relies on calcium ions. All muscle is innervated, although—as we will see—the part of the nervous system that innervates the muscle and the ability of the muscle to contract without nervous input varies from type to type.
Skeletal Muscle
Skeletal muscle is responsible for voluntary movement and is therefore innervated by the somatic nervous system. Due to the arrangement of actin and myosin into repeating units called sarcomeres, it appears striped or striated when viewed microscopically. Skeletal muscle is multinucleated because it is formed as individual muscle cells fuse into long rods during development.
There are multiple different types of fibers within skeletal muscle. Red fibers, also known as slow-twitch fibers, have high myoglobin content and primarily derive their energy aerobically. Myoglobin is an oxygen carrier that uses iron in a heme group to bind oxygen, imparting a red color. Red fibers also contain many mitochondria to carry out oxidative phosphorylation. White fibers, also known as fast-twitch fibers, contain much less myoglobin. Because there is less myoglobin, and therefore less iron, the color is lighter. These two types of fibers can be mixed in muscles. Muscles that contract slowly, but that can sustain activity (such as the muscles that support posture), contain a predominance of red fibers. Muscles that contract rapidly, but fatigue quickly, contain mostly white fibers.
REAL WORLD
Poultry provides a great example of the difference between red and white fibers. Most muscles of support, such as the thigh, are considered dark meat and contain a high concentration of red fibers. The pectoral muscles (breast meat), used by some poultry for only short bursts of flight, are considered white meat and have a high concentration of white fibers.
Smooth Muscle
Smooth muscle is responsible for involuntary action. Thus, smooth muscle is controlled by the autonomic nervous system. It is found in the respiratory tree, digestive tract, bladder, uterus, blood vessel walls, and many other locations. Smooth muscle cells have a single nucleus located in the center of the cell. Just like skeletal muscle, smooth muscle cells contain actin and myosin, but the fibers are not as well organized, so striations cannot be seen. Compared to skeletal muscle, smooth muscle is capable of more sustained contractions; a constant state of low-level contraction, as may be seen in the blood vessels, is called tonus. Smooth muscle can actually contract without nervous system input in what is known as myogenic activity. In this case, the muscle cells contract directly in response to stretch or other stimuli.
MCAT EXPERTISE
The MCAT loves to test the fact that both smooth and cardiac muscle exhibit myogenic activity. These muscle cells will respond to nervous input, but do not require external signals to undergo contraction.
Cardiac Muscle
Cardiac muscle has characteristics of both smooth and skeletal muscle types. Cardiac muscle is primarily uninucleated, but cells may contain two nuclei. Like smooth muscle, cardiac muscle contraction is involuntary and innervated by the autonomic nervous system. Unlike smooth muscle, cardiac muscle appears striated like skeletal.
One of the unique characteristics of cardiac muscle is how each cardiac myocyte communicates. Cardiac muscle cells are connected by intercalated discs, which contain many gap junctions. These gap junctions are connections between the cytoplasm of adjacent cells, allowing for the flow of ions directly between cells. This allows for rapid and coordinated depolarization of muscle cells and efficient contraction of cardiac muscle.
Cardiac muscle cells are able to define and maintain their own rhythm, termed myogenic activity. Starting at the sinoatrial (SA)node, depolarization spreads using conduction pathways to the atrioventricular (AV)node. From there, the depolarization spreads to the bundle of His and its branches, and then to the Purkinje fibers. The gap junctions allow for progressive depolarizations to spread via ion flow across the gap junctions between cells. The nervous and endocrine systems also play a role in the regulation of cardiac muscle contraction. The vagus nerve provides parasympathetic outflow to the heart and slows the heart rate. Norepinephrine from sympathetic neurons or epinephrine from the adrenal medulla binds to adrenergic receptors in the heart, causing an increased heart rate and greater contractility. One of the ways epinephrine does this is by increasing intracellular calcium levels within cardiac myocytes. Ultimately, cardiac contraction—like that of all types of muscle—relies on calcium.
The main characteristics of each muscle type are summarized in Table 11.1.
Table 11.1. Types of Muscle
SKELETAL MUSCLE CARDIAC MUSCLE SMOOTH MUSCLE
Striated Striated Nonstriated
Voluntary Involuntary Involuntary
Somatic innervation Autonomic innervation Autonomic innervation
Many nuclei per cell 1–2 nuclei per cell 1 nucleus per cell
Ca2+ required for contraction Ca2+ required for contraction Ca2+ required for contraction
Microscopic Structure of Skeletal Muscle
Each type of muscle has a specific microscopic structure. However, the MCAT tends to focus on the contractile elements and microscopic structure of skeletal muscle. In order to accurately answer those questions on Test Day, let’s take a moment to discuss skeletal muscle in detail.
The Sarcomere
The sarcomere is the basic contractile unit of skeletal muscle. Sarcomeres are made of thick and thin filaments. The thick filaments are organized bundles of myosin, whereas the thin filaments are made of actin along with two other proteins: troponin and tropomyosin. These proteins help to regulate the interaction between the actin and myosin filaments. Another protein, titin, acts as a spring and anchors the actin and myosin filaments together, preventing excessive stretching of the muscle.
MNEMONIC
To remember which filament is associated with troponin and tropomyosin, remember that actin has a T in it.
MNEMONIC
To remember which is the thin and thick filament, remember acthin: actin filaments are thin (while myosin filaments are thick).
Each sarcomere is divided into different lines, zones, and bands, as shown in Figure 11.1. Z-lines define the boundaries of each sarcomere. The M-line runs down the center of the sarcomere, through the middle of the myosin filaments. The I-band is the region containing exclusively thin filaments, whereas the H-zone contains only thick filaments. The A-band contains the thick filaments in their entirety, including any overlap with thin filaments. During contraction, the H-zone, I-band, the distance between Z-lines, and the distance between M-lines all become smaller, whereas the A-band’s size remains constant.
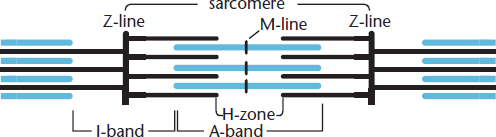
Figure 11.1. The Sarcomere Sarcomeres are the functional units of striated muscle.
MNEMONIC
Parts of the sarcomere:
- Z—Z is the end of the alphabet, and the end of the sarcomere
- M—Middle of the myosin filaments
- I—I is a thin letter (thin filaments only)
- H—H is a thick letter (thick filaments only)
- A—All of the thick filament, whether or not it is overlapping
Gross Structure of Myocytes
Sarcomeres are attached end-to-end to form myofibrils. Myofibrils are surrounded by a covering known as the sarcoplasmic reticulum (SR), a modified endoplasmic reticulum that contains a high concentration of Ca2+ ions. The sarcoplasm is a modified cytoplasm located just outside the sarcoplasmic reticulum. The cell membrane of a myocyte is known as the sarcolemma. The sarcolemma is capable of propagating an action potential and can distribute the action potential to all sarcomeres in a muscle using a system of transverse tubules (T-tubules) that are oriented perpendicularly to the myofibrils, as shown in Figure 11.2. Each myocyte, or muscle cell, contains many myofibrils arranged in parallel and can also be called a muscle fiber. The nuclei, of which there are many, are usually found at the periphery of the cell. Finally, many myocytes in parallel form a muscle.
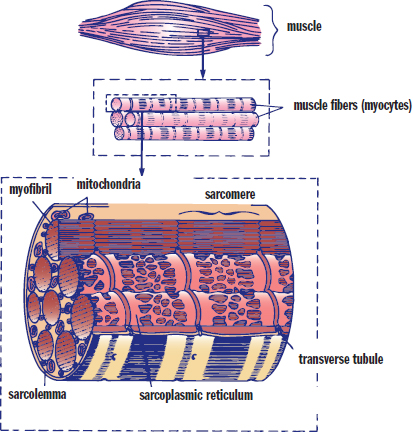
Figure 11.2. Architecture of Skeletal Muscle A muscle is composed of parallel myocytes (muscle fibers), which are composed of parallel myofibrils.
KEY CONCEPT
The sarcoplasmic reticulum is just a fancy name for the specialized endoplasmic reticulum in muscle cells.
KEY CONCEPT
A myofibril is an arrangement of many sarcomeres in series. A muscle fiber (or myocyte, or muscle cell) contains many myofibrils within it, arranged in parallel. A muscle is made up of parallel muscle fibers. These names are very similar; pay careful attention to terminology when reading about muscle structure!
Muscle Contraction
Contraction of muscle requires a series of coordinated steps that are repeated to induce further shortening. This process depends on both ATP and calcium.
Initiation
Contraction starts at the neuromuscular junction, where the nervous system communicates with muscles via motor (efferent)neurons. This signal travels down the neuron until it reaches the nerve terminal (synaptic bouton), where acetylcholine is released into the synapse. In the case of the neuromuscular junction, the nerve terminal can also be called the motor end plate. Acetylcholine binds to receptors on the sarcolemma, causing depolarization. Each nerve terminal controls a group of myocytes; together, the nerve terminal and its myocytes constitute a motor unit.
Depolarization triggers an action potential, which spreads down the sarcolemma to the T-tubules. The action potential travels down the T-tubules into the muscle tissues to the sarcoplasmic reticulum. When the action potential reaches the sarcoplasmic reticulum, Ca2+ is ultimately released. The calcium ions bind to a regulatory subunit in troponin, triggering a change in the confirmation of tropomyosin, to which troponin is bound. This change exposes the myosin-binding sites on the actin thin filament, as shown in Figure 11.3.
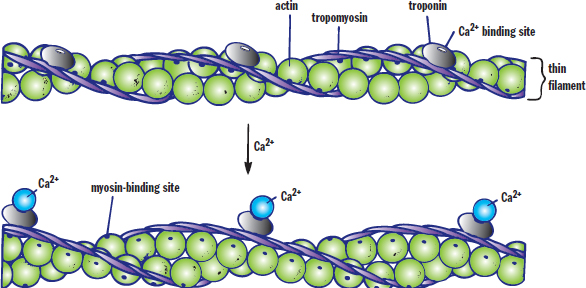
Figure 11.3. Regulation of Contraction with Calcium Calcium binds to troponin, leading to a conformational change in tropomyosin, which exposes the myosin-binding sites of actin.
Shortening of the Sarcomere
The free globular heads of the myosin molecules move toward and bind with the exposed sites on actin. The newly formed actin–myosin cross bridges then allow myosin to pull on actin, which draws the thin filaments toward the M-line, resulting in shortening of the sarcomere. The actin–myosin cross-bridge cycle is illustrated in Figure 11.4.
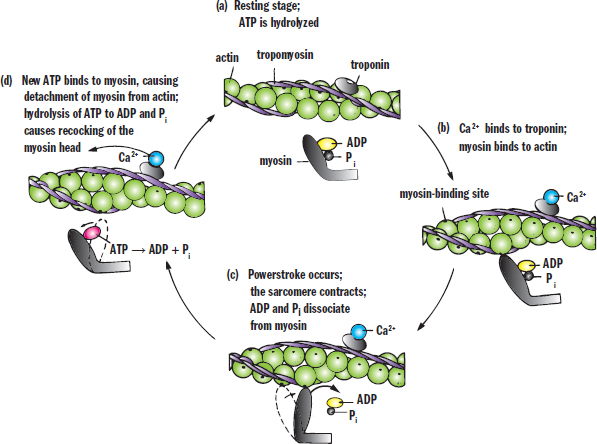
Figure 11.4. The Actin–Myosin Cross-Bridge Cycle Calcium and ATP are essential for muscle contraction and relaxation.
KEY CONCEPT
It is the dissociation of ADP and Pi from myosin that is responsible for the powerstroke, not the hydrolysis of ATP. The binding of ATP is required for releasing the myosin head from the actin filament.
Starting at the top of the diagram, myosin carrying hydrolyzed ATP (ADP and an inorganic phosphate, Pi) is able to bind with the myosin-binding site. The release of the inorganic phosphate and ADP in rapid succession provides the energy for the powerstroke and results in sliding of the actin filament over the myosin filament. Then, ATP binds to the myosin head, releasing it from actin. This ATP is hydrolyzed to ADP and Pi, which recocks the myosin head so that it is in position to initiate another cross-bridge cycle. The repetitive binding and releasing of myosin heads on actin filaments allows the thin filament to slide along the thick filament, causing sequential shortening of the sarcomere. This is known as the sliding filament model, as shown in Figure 11.5.
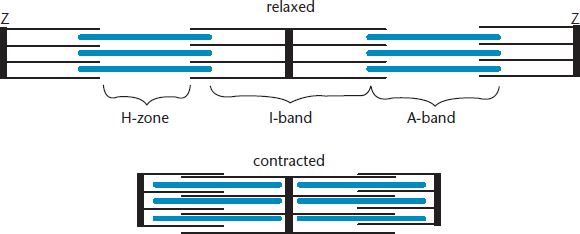
Figure 11.5. Sarcomere Contraction When a sarcomere contracts, both the H-zone and I-band shorten, while the A-band is unchanged.
Relaxation
Acetylcholine is degraded in the synapse by the enzyme known as acetylcholinesterase. This results in termination of the signal at the neuromuscular junction and allows the sarcolemma to repolarize. As the signal decays, calcium release ceases, and the SR takes up calcium from the sarcoplasm. The SR tightly controls intracellular calcium concentrations so that muscles are contracted only when necessary. ATP binds to the myosin heads, freeing them from actin. Once the myosin and actin disconnect, the sarcomere can return to its original width. Without calcium, the myosin-binding sites are covered by tropomyosin and contraction is prevented.
REAL WORLD
After death, ATP production ceases. Myosin heads cannot detach from actin, making it impossible for muscles to relax and lengthen. This condition is known as rigor mortis.
Stimulation, Summation, and Muscle Fatigue
Muscle cells, like neurons, exhibit an all-or-nothing response; either they respond completely to a stimulus or not at all. For muscle cells to respond, stimuli must reach a threshold value. The strength of a response from one muscle cell cannot be changed because the only options are all or nothing. Therefore, nerves control overall force by the number of motor units they recruit to respond. Maximal response occurs when all fibers within a muscle are stimulated to contract simultaneously.
BRIDGE
Why do muscle fibers contract in an all-or-nothing fashion? Because they are innervated by neurons that deliver signals using action potentials, which are all-or-nothing phenomena as well. Action potentials are discussed in Chapter 4 of MCAT Biology Review.
Simple Twitch
A simple twitch is the response of a single muscle fiber to a brief stimulus at or above threshold, as shown in Figure 11.6a. It consists of a latent period, contraction period, and relaxation period. The latent period is the time between reaching threshold and the onset of contraction. It is during this time that the action potential spreads along the muscle and allows for calcium to be released from the sarcoplasmic reticulum. The muscle then contracts, and, assuming calcium is cleared from the sarcoplasm, it then relaxes.
REAL WORLD
The disease tetanus is caused by a bacterium called Clostridium tetani that releases the toxin tetanospasmin. Tetanospasmin blocks the release of GABA from the neurons that inhibit motor neurons, making the motor neurons overexcitable. This leads to constant contraction of muscles, which can be so strong as to fracture bones. Tetanus can usually be prevented after exposure by administration of a tetanus immunoglobulin.
Summation and Tetanus
If a muscle fiber is exposed to frequent and prolonged stimulation, it will have insufficient time to relax. The contractions will combine, become stronger and more prolonged. This is known as frequency summation, as shown in Figure 11.6b. If the contractions become so frequent that the muscle is unable to relax at all, this is known as tetanus. Prolonged tetanus will result in muscle fatigue, explained below. Note that tetanus (the disease) includes tetanus (the physiological phenomenon) as one of its primary clinical features, but that tetanic physiology also occurs under normal circumstances with multiple simple twitches in succession.
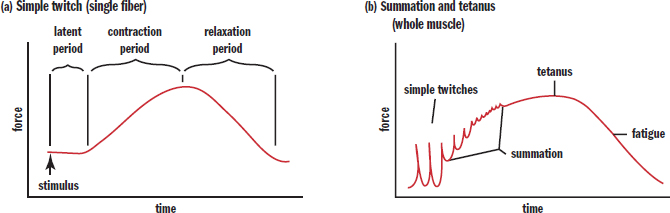
Figure 11.6. Force of Muscle Contraction Due to a Simple Twitch and Tetanus (a) A simple twitch contraction; (b) Summation of frequent simple twitches can lead to tetanus.
BIOLOGY GUIDED EXAMPLE WITH EXPERT THINKING
Study 1
Previous research has shown muscle tension generation is influenced by temperature of the muscle fibers. To further establish the connection between how temperature interacts with muscle tension generation, researchers measured the rate of tension rise at various temperatures. More specifically, researchers established change in the rate of tension rise is different at high temperatures (25 °C to 35 °C) and low temperatures (20 °C to 10 °C).
*IV: temperature
DV: muscle tension generation Experiment is trying to test the connection between temperature and tension*
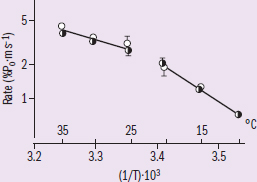
Figure 1 Tension generation rate versus temperature experiment results. Trend: Tension generation rate is lower and the slope of the line is more steep at lower temperatures Study 2
Another study is conducted that investigates the relationship between tetanic tension responses and temperature of the same type of muscle fibers. In this experiment, researchers directly observe the tension generation of the muscle plotted over time with electromyography sensor.
*There are two studies in the passage, the MCAT will likely ask for comparisons between the two IV: temperature again,
DV: tetanic tension responses (tetanic must be another type of tension)*
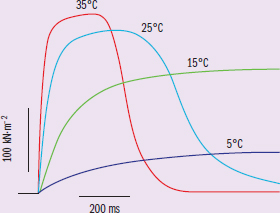
Figure 2 Tetanic tension responses obtained from one intact fiber bundle at four different temperatures, using suitable stimulation frequencies and duration.
Trend: as temperature decreases, the curve flattens out (i.e., change in tension remains low)
Adapted from Ranatunga K. W. (2018). Temperature effects on force and actin⁻myosin interaction in muscle: a look back on some experimental findings. International Journal of Molecular Sciences, 19(5), 1538. doi:10.3390/ijms19051538.
Does Study 2’s data conflict with Study 1’s data?
This question asks us whether two sets of data conflict with one another. To analyze this relationship, we need to draw the proper conclusions from each data set, and see how these two data sets are related. Conflict is when one data set reveals a relationship that is either not validated by similar data sets, or directly contradicted by similar data sets.
To start, we'll want to make sure we can understand each data set separately. The first study seeks to investigate how temperature affects the rate of tension generation by the muscle tissues. The results of this experiment are displayed as a line graph. One of the first things to look at when analyzing any figure are axes labels and their corresponding units. On the y-axis, we see the rate of tension rise. So, a higher value on that axis means the muscle can generate tension faster, or in other words, have a higher rate. For the x-axis, things are a bit more confusing. The axis displays temperature, but in two ways. Technically, it is the reciprocal of temperature, but fortunately for us the graph is also labeled with the corresponding real temperature location. Because of the reciprocal, higher temperatures are found closer to the left, and temperature decreases going toward the right. Besides this complication, the graph shows a pretty straightforward relationship. At higher temperatures (close to physiological temperature), the rate of tension rise is high, with the drop in rate from 35 °C to 25 °C being relatively minor. At lower temperatures, the rate of tension rise is much lower, and the change in rate as temperature decreases is more dramatic.
Study 2 examined a similar relationship between temperature and muscle tension. Here the graph shows a more visual representation of how the tension is generated in those muscles. From the shape of the curve, it appears that the measurement is for one stimulation, as the tension rises once and quickly tapers off. From the graph, we can make some quick observations. At higher temperatures, the max tension generated is higher, as well as the time required to reach peak tension. When temperature is lowered, muscle tension generation drops significantly.
To evaluate whether Study 2’s data conflicts with Study 1’s data, we need to compare and assess how the two data sets are related. Both of these graphs have temperature as the independent variable, so we must look at what each data set demonstrates with that change in temperature. Study 1 shows a rise in rate of tension. While Study 2 does not report rate of tension rise explicitly, it does show tension over time, which is essentially rate! At 35 °C and 25 °C, the slope of tension increase is sharp, meaning that the rate of tension increase is high. At lower temperature, the slope is more gentle, and tension generation takes significantly longer. This means that Study 2 corroborates Study 1’s data in that higher temperature is correlated with a higher rate, while lower temperature is correlated with lower rate.
What about the change in rate? How is that visualized? Study 1 shows that change in the rate of tension rise at high temperature is more mild than the change in rate at lower temperatures. From Study 2’s graph, we can see that from 35 °C to 25 °C, the change in the slope (and therefore rate) of the tension is rather small. However, the change in slope between 15 °C and 5 °C is much more dramatic. Since we know that the slope represents the rate of tension rise, the change in slope must represent the change in rate.
Thus, Study 2 does not conflict with Study 1. In fact, the two studies corroborate each other!
Oxygen Debt and Muscle Fatigue
Muscles require ATP to function. Slow-twitch (red) muscle fibers have high levels of mitochondria and thus use oxidative phosphorylation to make ATP. However, this means that high concentrations of oxygen are required to generate the large amounts of ATP muscle cells need. There are two supplemental energy reserves in muscle. Creatine phosphate is created by transferring a phosphate group from ATP to creatine during times of rest. This reaction can then be reversed during muscle use to quickly generate ATP from ADP:
creatine + ATP ⇌ creatine phosphate + ADP
Muscle also contains myoglobin, which binds oxygen with high affinity. As exercising muscles run out of oxygen, they use myoglobin reserves to keep aerobic metabolism going. Fast-twitch (white) muscle fibers have fewer mitochondria and must rely on glycolysis and fermentation to make ATP under most circumstances. When a person exercises, heart rate and respiratory rate increase in order to move more oxygen to actively respiring muscles. The oxyhemoglobin dissociation curve undergoes a right shift in the presence of increased carbon dioxide concentration, increased hydrogen ion concentration (decreased pH), and increased temperature. However, even with these adaptations, muscle use can quickly overwhelm the ability of the body to deliver oxygen. Then, even red muscle fibers must switch to anaerobic metabolism and produce lactic acid, at which point the muscle begins to fatigue. The difference between the amount of oxygen needed by the muscles and the actual amount present is called the oxygen debt. After the cessation of strenuous exercise, the body must metabolize all of the lactic acid it has produced. Most lactic acid is converted back into pyruvate, which can enter the citric acid cycle. This process requires oxygen, and the amount of oxygen required to recover from strenuous exercise is equal to the oxygen debt.
MCAT CONCEPT CHECK 11.1
Before you move on, assess your understanding of the material with these questions.
- What type(s) of muscle (skeletal, smooth, or cardiac) does each of the following describe? (Note: Circle the correct response(s) next to each item.)
Skeletal Smooth Cardiac
- Striated:
Skeletal Smooth Cardiac
- Always uninucleated:
Skeletal Smooth Cardiac
- Always polynucleated:
Skeletal Smooth Cardiac
- Voluntary:
Skeletal Smooth Cardiac
- Innervated by the autonomic nervous system:
Skeletal Smooth Cardiac
- Exhibits myogenic activity:
- Which zone or band in the sarcomere does NOT change its length during muscle contraction? Why?
- What are the events that initiate muscle contraction, in order? Start with neurotransmitter release and trace the pathway to the point where myosin binds with actin.
- What role does the binding of ATP to the myosin head play in the cross-bridge cycle? What about the dissociation of ADP and inorganic phosphate from the myosin head?
- Binding of ATP:
- Dissociation of ADP and inorganic phosphate:
- What is tetanus (the physiological phenomenon, not the disease)?
11.2 The Skeletal System
LEARNING OBJECTIVES
After Chapter 11.2, you will be able to:
- Distinguish between compact and spongy bone
- Identify the three structural parts of a bone and their relative contributions to growth
- Recall the major chemical component of bone
- Describe the function(s) of osteoblasts, osteoclasts, and chondrocytes
- Name the substance that lubricates movable joints and where it is produced
There are two types of skeletons: exoskeletons and endoskeletons. Exoskeletons encase whole organisms and are usually found in arthropods, such as crustaceans and insects. Vertebrates, including humans, have endoskeletons. Endoskeletons are internal, but are not able to protect the soft tissue structures as well as exoskeletons. However, exoskeletons must be shed and regrown to accommodate growth. Endoskeletons are much better able to accommodate the growth of a larger organism.
Skeletal Structure
The components of our skeletal system are divided into axial and appendicular skeletons. The axial skeleton consists of the skull, vertebral column, rib cage, and hyoid bone (a small bone in the anterior neck used for swallowing); it provides the basic central framework for the body. The appendicular skeleton consists of the bones of the limbs (humerus, radius and ulna, carpals, metacarpals, and phalanges in the upper limb; and femur, tibia and fibula, tarsals, metatarsals, and phalanges in the lower limb); the pectoral girdle (scapula and clavicle); and pelvis. Both skeleton types are covered by other structures (muscle, connective tissue, and vasculature). The structure of the skeleton is shown in Figure 11.7, with many of the bones labeled (individual bones are labeled in red).
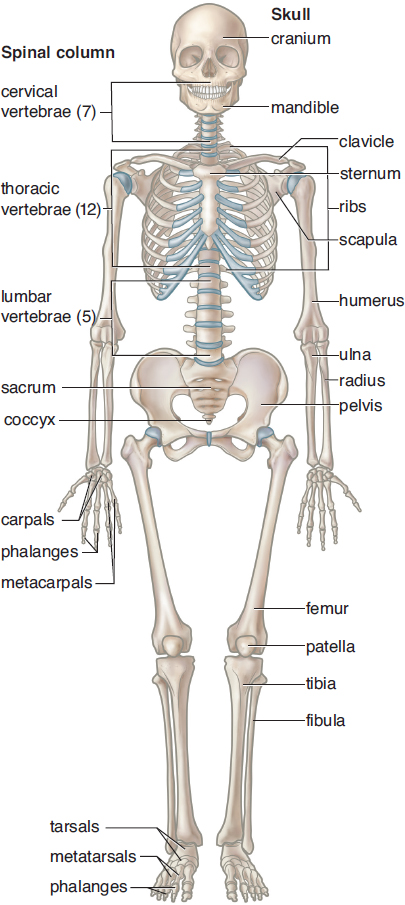
Figure 11.7. Anatomy of the Human Skeleton
The skeleton is created from two major components: bone and cartilage.
REAL WORLD
An adult human has 206 bones. Over 100 of these are in the hands and feet.
Bone Composition
Bone is a connective tissue derived from embryonic mesoderm. Bone is much harder than cartilage, but is relatively lightweight.
Macroscopic Bone Structure
The structure of bone can be seen in Figure 11.8.
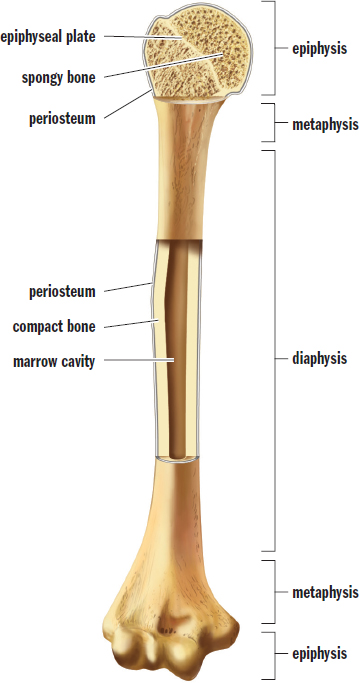
Figure 11.8. Anatomy of a Long Bone (Humerus)
Bone’s characteristic strength comes specifically from compact bone. It lives up to its name, as it is both dense and strong. The other type of bone structure is spongy or cancellous bone. The lattice structure of spongy bone is visible under microscopy and consists of bony spicules (points) known as trabeculae. The cavities between trabeculae are filled with bone marrow, which may be either red or yellow. Red marrow is filled with hematopoietic stem cells, which are responsible for the generation of all the cells in our blood; yellow marrow is composed primarily of fat and is relatively inactive.
Bones in the appendicular skeleton are typically long bones, which are characterized by cylindrical shafts called diaphyses that swell at each end to form metaphyses, and that terminate in epiphyses. The outermost portions of bone are composed of compact bone, whereas the internal core is made of spongy bone. Long bone diaphyses and metaphyses are full of bone marrow. The epiphyses, on the other hand, use their spongy cores for more effective dispersion of force and pressure at the joints. At the internal edge of the epiphysis is an epiphyseal (growth) plate, which is a cartilaginous structure and the site of longitudinal growth. Prior to adulthood, the epiphyseal plate is filled with mitotic cells that contribute to growth; during puberty, these epiphyseal plates close and vertical growth is halted. Finally, a fibrous sheath called the periosteum surrounds the long bone to protect it as well as serve as a site for muscle attachment. Some periosteal cells are capable of differentiating into bone-forming cells; a healthy periosteum is necessary for bone growth and repair.
Structures in the musculoskeletal system are held together with dense connective tissue. Tendons attach muscle to bone and ligaments hold bones together at joints.
BRIDGE
The root lig– comes from Latin, where it means to “to tie; bind.” Think of DNA ligase, discussed in Chapter 6 of MCAT Biochemistry Review. Think of ligands in complex ions, discussed in Chapter 9 of MCAT General Chemistry Review. In this case, ligaments tie bones to each other to stabilize joints.
Microscopic Bone Structure
The strength of compact bone comes from the bone matrix, which has both organic and inorganic components. The organic components include collagen, glycoproteins, and other peptides. The inorganic components include calcium, phosphate, and hydroxide ions, which harden together to form hydroxyapatite crystals (Ca10(PO4)6(OH)2). Minerals such as sodium, magnesium, and potassium are also stored in bone.
Strong bones require uniform distribution of organic and inorganic materials. The bony matrix is ordered into structural units known as osteons or Haversian systems, as shown in Figure 11.9. Each of these osteons contains concentric circles of bony matrix called lamellae surrounding a central microscopic channel. Longitudinal channels (those with an axis parallel to the bone) are known as Haversian canals, while transverse channels (those with an axis perpendicular to the bone) are known as Volkmann’s canals. These canals contain the blood vessels, nerve fibers, and lymph vessels that maintain the health of the bone. Between the lamellar rings are small spaces called lacunae, which house mature bone cells known as osteocytes. The lacunae are interconnected by tiny channels called canaliculi that allow for the exchange of nutrients and wastes between osteocytes and the Haversian and Volkmann’s canals.
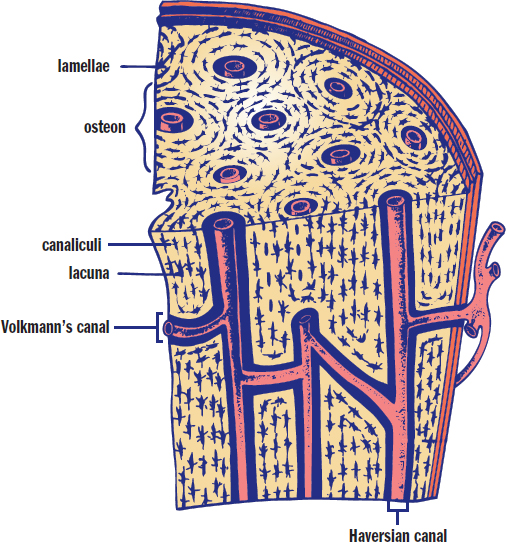
Figure 11.9. Bone Matrix Cross-sectional and longitudinal views highlighting Haversian systems
KEY CONCEPT
Bone appears to be rigid and static, but it is actually quite dynamic. It is both vascular and innervated, which is why it hurts so much to break a bone. In addition, bone remains in a vigorous equilibrium between construction and destruction, known as bone remodeling.
REAL WORLD
Osteoporosis is the most common bone disease in the United States. It is thought to be the result of increased osteoclast resorption and some concomitant slowing of bone formation, both of which lead to loss of bone mass. Estrogen is believed to help prevent osteoporosis by stimulating osteoblast activity.
Bone Remodeling
Two cell types are largely responsible for building and maintaining strong bones: osteoblasts and osteoclasts. Osteoblasts build bone, whereas osteoclasts, polynucleated resident macrophages of bone, resorb it. These processes together contribute to the constant turnover of bone, as shown in Figure 11.10. During bone formation, essential ingredients such as calcium and phosphate are obtained from the blood. During bone resorption, these ions are released back into the bloodstream. Bone remodeling occurs in response to stress, and bone actually remodels in such a way as to accommodate the repetitive stresses faced by the body. Endocrine hormones may also affect bone metabolism. Parathyroid hormone, a peptide hormone released by the parathyroid glands in response to low blood calcium, promotes resorption of bone, increasing the concentration of calcium and phosphate in the blood. Vitamin D, which is activated by parathyroid hormone, also promotes the resorption of bone. This may seem counterintuitive at first—isn’t vitamin D used to promote bone growth? Indeed, the resorption of bone in response to vitamin D actually encourages the growth of new, stronger bone, thus overcompensating for the effect of resorbing bone in the first place. Finally, calcitonin, a peptide hormone released by the parafollicular cells of the thyroid in response to high blood calcium, promotes bone formation, lowering blood calcium levels.
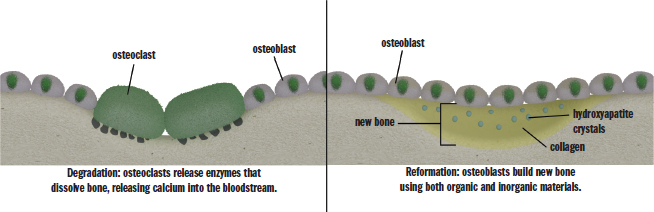
Figure 11.10. Bone Remodeling
MNEMONIC
Osteoblasts build bone. Osteoclasts chew bone.
Cartilage
Cartilage is softer and more flexible than bone. Cartilage consists of a firm but elastic matrix called chondrin that is secreted by cells called chondrocytes. Fetal skeletons are mostly made up of cartilage. This is advantageous because fetuses must grow and develop in a confined environment and then must traverse the birth canal. Adults have cartilage only in body parts that need a little extra flexibility or cushioning (external ear, nose, walls of the larynx and trachea, intervertebral discs, and joints). Cartilage also differs from bone in that it is avascular (without blood and lymphatic vessels) and is not innervated.
Most of the bones of the body are created by the hardening of cartilage into bone. This process is known as endochondral ossification and is responsible for the formation of most of the long bones of the body. Bones may also be formed through intramembranous ossification, in which undifferentiated embryonic connective tissue (mesenchymal tissue) is transformed into, and replaced by, bone. This occurs in bones of the skull.
Joints and Movement
Like bone and cartilage, joints are also made of connective tissue and come in two major varieties: immovable and movable. Immovable joints consist of bones that are fused together to form sutures or similar fibrous joints. These joints are found primarily in the head, where they anchor bones of the skull together.
Movable joints, structures of which are shown in Figure 11.11, include hinge joints (like the elbow or knee), ball-and-socket joints (like the shoulder or hip), and others. They permit bones to shift relative to one another. Movable joints are strengthened by ligaments, which are pieces of fibrous tissue that connect bones to one another, and consist of a synovial capsule, which encloses the actual joint cavity (articular cavity). A layer of soft tissue called the synovium secretes synovial fluid, which lubricates the movement of structures in the joint space. The articular cartilage contributes to the joint by coating the articular surfaces of the bones so that impact is restricted to the lubricated joint cartilage, rather than to the bones.
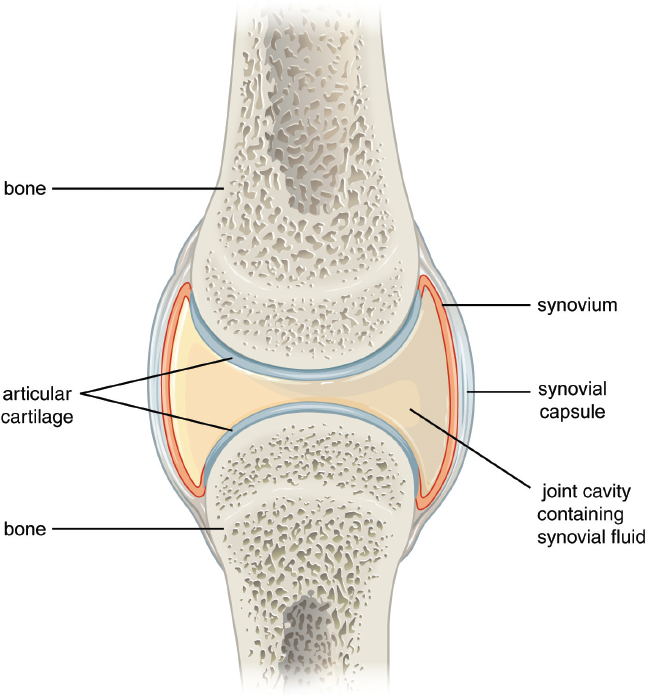
Figure 11.11. Structures in a Movable Joint
REAL WORLD
Degradation of articular cartilage (cartilage in joints) can lead to medical issues like osteoarthritis. Osteoarthritis (or “arthritis” in the lay population) is painful because a lack of cartilage in joints leads to bones rubbing directly on one another.
When a muscle is attached to two bones, its contraction will cause one of the bones to move. The end of the muscle with a larger attachment to bone (usually the proximal connection) is called the origin. The end with the smaller attachment to bone (usually the distal connection) is called the insertion. Often, our muscles work in antagonistic pairs; one relaxes while the other contracts. Such is the case in the arm, where the biceps brachii and triceps brachii work antagonistically, as shown in Figure 11.12. When the biceps contracts and the triceps relaxes, the elbow is flexed; when the triceps contracts and the biceps relaxes, the elbow is extended. Muscles can also be synergistic—working together to accomplish the same function.
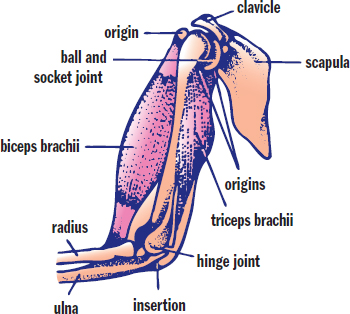
Figure 11.12. Antagonistic Muscle Pairs The biceps brachii and triceps brachii are an example of a muscle pair that works antagonistically; the contraction of one causes the other to elongate.
Muscles may also be classified by the types of movements they coordinate. A flexor muscle decreases the angle across a joint (like the biceps brachii); an extensor increases or straightens this angle (like the triceps brachii). An abductor moves a part of the body away from the midline (like the deltoid); an adductor moves a part of the body toward the midline (like the pectoralis major). Medial and lateral rotation describe motions that occur in limbs; a medial rotator rotates the axis of the limb toward the midline (like the subscapularis), whereas a lateral rotator rotates the axis of the limb away from the midline (like the infraspinatus).
MCAT CONCEPT CHECK 11.2
Before you move on, assess your understanding of the material with these questions.
- What is the difference between compact and spongy bone?
- Compact bone:
- Spongy bone:
- What are the three structural parts of a bone? Which part contributes most to linear growth?
- What chemical forms most of the inorganic component of bone?
- What are the functions of osteoblasts, osteoclasts, and chondrocytes?
- Osteoblast:
- Osteoclast:
- Chondrocyte:
- What liquid provides the lubrication for movable joints? What tissue produces it?
Conclusion
One concept that has been emphasized throughout the past eight chapters on anatomy and physiology is the notion that organ systems work together in order to achieve a desired effect. The musculoskeletal system is no different. Usually, we think of the musculoskeletal system as being responsible for movement, but to limit the musculoskeletal system to that function would be shortsighted. The bones are reservoirs of calcium and other minerals that can be released through hormonal signaling. They protect the internal organs and provide support for the body. Muscle tissue not only moves these bones, but pumps blood through the body and is key to the function of a number of other systems, including respiration, digestion, blood pressure and vascular tone, and reproduction and childbirth. As you review anatomy and physiology and master the fundamentals of each organ system, be sure to pay special attention to how each organ system interacts with the others. While the MCAT expects you to understand each individual organ system, it will also challenge you by asking you to think critically about how one system impacts another. By spending some time in your studies looking at these interactions, you will be one step ahead on Test Day.
In our final chapter of MCAT Biology Review, we will switch gears and look at the transfer of information from generation to generation. This picks up on a discussion from the first three chapters of the book in which we explored the organization of cells and their genetic material, reproduction, and embryogenesis and development. In the next chapter, we’ll describe classical (Mendelian) inheritance and conclude with a note on how the gene pool can change over time with the topic of evolution.
GO ONLINE
You've reviewed the content, now test your knowledge and critical thinking skills by completing a test-like passage set in your online resources!
CONCEPT SUMMARY
The Muscular System
- There are three main types of muscle: skeletal muscle, smooth muscle, and cardiac muscle.
- Skeletal muscle is involved in support and movement, propulsion of blood in the venous system, and thermoregulation. It appears striated, is under voluntary (somatic) control, is polynucleated, and can be divided into red (slow-twitch) fibers that carry out oxidative phosphorylation and white (fast-twitch) fibers that rely on anaerobic metabolism.
- Smooth muscle is in the respiratory, reproductive, cardiovascular, and digestive systems. It appears nonstriated, is under involuntary (autonomic) control, and is uninucleated. It can display myogenic activity, or contraction without neural input.
- Cardiac muscle comprises the contractile tissue of the heart. It appears striated, is under involuntary (autonomic) control, and is uninucleated (sometimes binucleated). It can also display myogenic activity. Cells are connected with intercalated discs that contain gap junctions.
- The sarcomere is the basic contractile unit of striated muscle.
- Sarcomeres are made of thick (myosin) and thin (actin) filaments.
- Troponin and tropomyosin are found on the thin filament and regulate actin–myosin interactions.
- The sarcomere can be divided into different lines, zones, and bands.
- The boundaries of each sarcomere are defined by Z-lines.
- The M-line is located in the middle of the sarcomere.
- The I-band contains only thin filaments.
- The H-zone consists of only thick filaments.
- The A-band contains the thick filaments in their entirety. It is the only part of the sarcomere that maintains a constant size during contraction.
- Sarcomeres attach end-to-end to become myofibrils, and each myocyte (muscle cell or muscle fiber) contains many myofibrils.
- Myofibrils are surrounded by the sarcoplasmic reticulum, a calcium-containing modified endoplasmic reticulum, and the cell membrane of a myocyte is known as the sarcolemma.
- A system of T-tubules is connected to the sarcolemma and oriented perpendicularly to the myofibrils, allowing the action potential to reach all parts of the muscle.
- Muscle contraction begins at the neuromuscular junction, where the motor neuron releases acetylcholine that binds to receptors on the sarcolemma, causing depolarization.
- This depolarization spreads down the sarcolemma to the T-tubules, triggering the release of calcium ions.
- Calcium binds to troponin, causing a shift in tropomyosin and exposure of the myosin-binding sites on the actin thin filament.
- Shortening of the sarcomere occurs as myosin heads bind to the exposed sites on actin, forming cross bridges and pulling the actin filament along the thick filament, which results in contraction. This is known as the sliding filament model.
- The muscle relaxes when acetylcholine is degraded by acetylcholinesterase, terminating the signal and allowing calcium to be brought back into the SR. ATP binds to the myosin head, allowing it to release from actin.
- Muscle cells exhibit an all-or-nothing response called a simple twitch.
- Addition of multiple simple twitches before the muscle has an opportunity to fully relax is called frequency summation.
- Simple twitches that occur so frequently as to not let the muscle relax at all can lead to tetanus, a more prolonged and stronger contraction.
- Muscle cells have additional energy reserves to reduce oxygen debt (the difference between the amount of oxygen needed and the amount present) and forestall fatigue.
- Creatine phosphate can transfer a phosphate group to ADP, forming ATP.
- Myoglobin is a heme-containing protein that is a muscular oxygen reserve.
The Skeletal System
- Internal skeletons (like those in humans) are called endoskeletons; external skeletons (like those in arthropods) are called exoskeletons.
- The human skeletal system can be divided into axial and appendicular skeletons.
- The axial skeleton consists of structures in the midline such as the skull, vertebral column, rib cage, and hyoid bone.
- The appendicular skeleton consists of the bones of the limbs, the pectoral girdle, and the pelvis.
- Bone is derived from embryonic mesoderm and includes both compact and spongy (cancellous) types.
- Compact bone provides strength and is dense.
- Spongy or cancellous bone has a lattice-like structure consisting of bony spicules known as trabeculae. The cavities are filled with bone marrow.
- Long bones contain shafts called diaphyses that flare to form metaphyses and terminate in epiphyses. The epiphysis contains an epiphyseal (growth) plate that causes linear growth of the bone.
- Bone is surrounded by a layer of connective tissue called periosteum.
- Bones are attached to muscles by tendons and to each other by ligaments.
- Bone matrix has both organic components, like collagen, glycoproteins, and other peptides; and inorganic components, like hydroxyapatite.
- Bone is organized into concentric rings called lamellae around a central Haversian or Volkmann’s canal. This structural unit is called an osteon or Haversian system.
- Between lamellar rings are lacunae, where osteocytes reside, which are connected with canaliculi to allow for nutrient and waste transfer.
- Bone remodeling is carried out by osteoblasts and osteoclasts. Osteoblasts build bone, while osteoclasts resorb bone.
- Parathyroid hormone increases resorption of bone, increasing calcium and phosphate concentrations in the blood.
- Vitamin D also increases resorption of bone, leading to increased turnover and, subsequently, the production of stronger bone.
- Calcitonin increases bone formation, decreasing calcium concentrations in the blood.
- Cartilage is a firm, elastic material secreted by chondrocytes. Its matrix is called chondrin.
- Cartilage is usually found in areas that require more flexibility or cushioning.
- Cartilage is avascular and is not innervated.
- In fetal life, bone forms from cartilage through endochondral ossification. Some bones, especially those of the skull, form directly from undifferentiated tissue (mesenchyme) in intramembranous ossification.
- Joints may be classified as immovable or movable.
- Immovable joints are fused together to form sutures or similar fibrous joints.
- Movable joints are usually strengthened by ligaments and contain a synovial capsule.
- Synovial fluid, secreted by the synovium, aids in motion by lubricating the joint.
- Each bone in the joint is coated with articular cartilage to aid in movement and provide cushioning.
- Muscles that serve opposite functions come in antagonistic pairs; when one muscle contracts, the other lengthens.
ANSWERS TO CONCEPT CHECKS
**11.1**
- Skeletal and cardiac muscle are striated. Smooth muscle is always uninucleated. Skeletal muscle is always polynucleated. Skeletal muscle is voluntary. Smooth and cardiac muscle are innervated by the autonomic nervous system. Smooth and cardiac muscle exhibit myogenic activity.
- The A-band does not change length during muscle contraction because it is the entire length of the myosin filament. The filaments do not change length, but rather slide over each other; thus, the A-band should remain a constant length during contraction.
- Release of acetylcholine from motor neuron → activation of acetylcholine receptors in sarcolemma → depolarization of sarcolemma → spreading of signal using T-tubules → release of calcium from sarcoplasmic reticulum (SR) → binding of calcium to troponin → conformational shift in tropomyosin → exposure of myosin-binding sites → myosin binds to actin
- ATP binding allows the myosin filament to disconnect from actin. Dissociation of ADP and inorganic phosphate from myosin causes the powerstroke.
- Tetanus is the summation of multiple simple twitches that occur too quickly for the muscle to relax. This leads to a stronger and more prolonged contraction of the muscle.
**11.2**
- Compact bone is dense and is used for its strength; it forms most of the outer layers of a bone. Spongy (cancellous) bone has many spaces between bony spicules called trabeculae and is the site of marrow production. It is found in the interior core of the bone and also helps distribute forces or pressures on the bone.
- The three parts of a bone are the diaphysis, metaphysis, and epiphysis. Growth plates are found in epiphyses and contribute to linear growth.
- Most inorganic bone is composed of hydroxyapatite crystals.
- Osteoblasts build bone. Osteoclasts “chew” bone (break it down). Chondrocytes form cartilage.
- Synovial fluid, produced by the synovium, lubricates movable joints.
SCIENCE MASTERY ASSESSMENT EXPLANATIONS
1. D
We are given a diagram of a sarcomere and asked to determine which regions shorten during muscle contraction. All bands and zones of the sarcomere shorten during contraction except the A-band, which is the full length of the thick filaments. In this diagram, that is region 1. Thus, the remaining regions all shorten, making (D) the correct answer. Region 2 represents the I-band, region 3 represents the H-zone, and region 4 is the length of the sarcomere between Z-lines.
2. C
Region 1 contains both thick and thin filaments overlapping each other. This region refers to the A-band and is measured from one end of the thick filaments to the other. This is also the only portion of the sarcomere that does not change length during muscle contraction.
3. D
The sarcomere is the contractile unit in striated muscle cells. One sarcomere is represented by the area between the two vertical lines, referred to as the Z-lines. In addition, the Z-lines anchor the thin filaments. In the diagram, a sarcomere is therefore defined by region 4.
4. C
Calcium is released from the sarcoplasmic reticulum into the sarcoplasm. It binds the troponin molecules on the thin filaments, causing the strands of tropomyosin to shift, thereby exposing the myosin-binding sites on the thin filaments.
5. A
Let’s quickly define each one of the four cells discussed in the answer choices. Osteoblasts are bone cells involved in the secretion of bone matrix, as (A) states. Osteoclasts are large, polynucleated cells involved in bone resorption. Osteocytes are mature bone cells that eventually become surrounded by their matrix; their primary role is bone maintenance. Finally, chondrocytes are cells that secrete chondrin, an elastic matrix that makes up cartilage.
6. C
This question is essentially asking where longitudinal growth occurs in bones. The most likely site of abnormalities in this child’s femur is the epiphyseal plate, a disc of cartilaginous cells at the internal border of the epiphysis, because the epiphyseal plate is the site of longitudinal growth. Damage to the epiphysis (with or without metaphysis involvement) can imply damage to the epiphyseal plate.
7. D
Red fibers are slow-twitching fibers that have high levels of myoglobin and many mitochondria. They derive their energy from aerobic respiration and are capable of sustained vigorous activity. This eliminates (A) and (B). White fibers, on the other hand, are fast-twitching fibers and contain lower levels of myoglobin and fewer mitochondria. Because of their composition, they derive more of their energy anaerobically and fatigue more easily. This eliminates (C) and makes (D) the correct answer.
8. A
The articular surfaces of the bones are covered with a layer of smooth articular cartilage. The epiphysis is a portion of the bone itself, eliminating (B). Synovial fluid lubricates the movement in the joint space, but does not stop the bones from contacting one another; this is the job of articular cartilage, eliminating (C). There is no appreciable function for smooth muscle in the joint space, eliminating (D).
9. B
The only type of muscle that is always multinucleated is skeletal muscle, making (B) the correct answer. Cardiac muscle may contain one or two centrally located nuclei, so Statement I is incorrect. Smooth muscle, on the other hand, always has only one centrally located nucleus.
10. D
Myogenic activity refers to the ability of a muscle to contract without nervous stimulation, such as in response to other stimuli like stretching. Smooth and cardiac muscle both possess myogenic activity.
11. D
Yellow marrow is largely inactive and is infiltrated by adipose tissue, making (D) the correct answer.
12. D
The periosteum, a fibrous sheath that surrounds long bones, is the site of attachment to muscle tissue. Some periosteum cells are capable of differentiating into bone-forming cells called osteoblasts. This eliminates (A), (B), and (C). It is the synovium that secretes fluid into the joint cavity (joint space), not the periosteum, making (D) the correct answer.
13. D
The axial skeleton includes the skull, vertebral column, rib cage, and hyoid bone. The sternum is a point of attachment of the rib cage and is thus a part of the axial, not appendicular, skeleton. The limb bones, pectoral girdle, and pelvis are all part of the appendicular skeleton.
14. B
Bones form in one of two ways: endochondral ossification and intramembranous ossification. Endochondral ossification is the replacement of cartilage with bone and occurs mostly in long bones, eliminating (A). Intramembranous ossification is the formation of bone from undifferentiated connective tissue cells (mesenchyme) and occurs mostly in the skull, making (B) the correct answer. Bone resorption is the breakdown of bone, not its formation, eliminating (C). Longitudinal growth occurs in long bones and is responsible for increasing height over time, but does not play a role in fontanelle ossification, eliminating (D).
15. C
An unprovoked fracture of the hip is not a normal finding in a person who is younger. Given that the patient has a high calcium level, it is likely that the patient has an increased level of bone resorption that is causing the bones to be more fragile. Parathyroid hormone causes calcium release from bones. If this patient had an overactive parathyroid gland—or even cancer in this gland—then it is likely that calcium could still be resorbed from the bones even though blood calcium levels are already high.
GO ONLINE
Consult your online resources for additional practice.
SHARED CONCEPTS
Biology Chapter 4
The Nervous System
Biology Chapter 5
The Endocrine System
Biology Chapter 6
The Respiratory System
Biology Chapter 7
The Cardiovascular System
General Chemistry Chapter 9
Solutions
Physics and Math Chapter 1
Kinematics and Dynamics