Chapter 7: Psychological Disorders
Chapter 7: Psychological Disorders
SCIENCE MASTERY ASSESSMENT
Every pre-med knows this feeling: there is so much content I have to know for the MCAT! How do I know what to do first or what’s important?
While the high-yield badges throughout this book will help you identify the most important topics, this Science Mastery Assessment is another tool in your MCAT prep arsenal. This quiz (which can also be taken in your online resources) and the guidance below will help ensure that you are spending the appropriate amount of time on this chapter based on your personal strengths and weaknesses. Don’t worry though—skipping something now does not mean you’ll never study it. Later on in your prep, as you complete full-length tests, you’ll uncover specific pieces of content that you need to review and can come back to these chapters as appropriate.
How to Use This Assessment
If you answer 0–7 questions correctly:
Spend about 1 hour to read this chapter in full and take limited notes throughout. Follow up by reviewing all quiz questions to ensure that you now understand how to solve each one.
If you answer 8–11 questions correctly:
Spend 20–40 minutes reviewing the quiz questions. Beginning with the questions you missed, read and take notes on the corresponding subchapters. For questions you answered correctly, ensure your thinking matches that of the explanation and you understand why each choice was correct or incorrect.
If you answer 12–15 questions correctly:
Spend less than 20 minutes reviewing all questions from the quiz. If you missed any, then include a quick read-through of the corresponding subchapters, or even just the relevant content within a subchapter, as part of your question review. For questions you answered correctly, ensure your thinking matches that of the explanation and review the Concept Summary at the end of the chapter.
- Which of the following is an example of a negative symptom seen in schizophrenia?
- Auditory hallucinations
- Disorganized behavior
- Disturbance of affect
- Delusions
- During an interview with a schizophrenic patient, a psychiatrist notices that the patient keeps repeating what the psychiatrist says. This phenomenon is known as:
- echolalia.
- echopraxia.
- loosening of associations.
- neologisms.
- A 42-year-old patient has always been extremely neat and tidy. This person works as a secretary and stays long after normal working hours to check the punctuation and spelling of letters prepared during the day. The patient was referred for counseling by a supervisor after repeatedly getting into fights with coworkers. “They don’t take the job to heart,” the patient says. “They just joke around all day.” The most likely preliminary diagnosis for this patient is:
- obsessive–compulsive personality disorder.
- antisocial personality disorder.
- narcissistic personality disorder.
- borderline personality disorder.
- Which of the following is true with regard to a major depressive episode?
- It may last less than two weeks.
- It must involve thoughts of suicide or a suicide attempt.
- It may involve a decrease in sleep.
- It must involve feelings of sadness.
- A young person moves to a new city to start work on an accelerated degree program. After a few months this individual visits the doctor complaining of stress and isolation and is diagnosed with depression. The doctor ascribes the cause to low levels of serotonin and prescribes an SSRI for treatment. Which of the following best describes the physician’s approach to diagnosis and treatment?
- Biomedical approach with indirect therapy
- Biomedical approach with direct therapy
- Biopsychosocial approach with indirect therapy
- Biopsychosocial approach with direct therapy
- A young person of unknown age is brought by the Philadelphia police to the local emergency department for evaluation after being found wandering in a park. The patient carries no identification and is unable to provide a first or last name or any life details, except that the name Phoenix seems familiar. The police in Arizona are contacted and find a missing persons report matching the patient’s description. Based on this information, the most likely diagnosis for this patient is:
- depersonalization/derealization disorder.
- dissociative identity disorder.
- somatic symptom disorder.
- dissociative amnesia with dissociative fugue.
- In addition to being a freestanding diagnosis, agoraphobia is most often seen in association with which other psychiatric diagnosis?
- Obsessive–compulsive disorder
- Avoidant personality disorder
- Generalized anxiety disorder
- Panic disorder
- A researcher is interested in studying fear responses to a variety of different stimuli. To rule out potential confounding variables, the research excludes individuals with phobias from the study. In a sample of 50 participants, how many will likely be excluded from the study, assuming that the sample is representative of the overall population?
- 45
- 15
- 10
- 5
Questions 9–10 refer to the scenario described below.
A physician is attempting to diagnose a patient’s mental disorder based on a set of symptoms. The confirmed symptoms currently include appetite disturbance, substantial weight change, decreased energy, a feeling of worthlessness, and excessive guilt.
- What two disorders could these symptoms indicate?
- Major depressive and bipolar disorders
- Dissociative amnesia and depersonalization/derealization disorder
- Alzheimer’s disease and Parkinson’s disease
- Specific phobia and panic disorder
- What should the physician ask about to distinguish between the two possible disorders affecting that patient?
- Whether the patient has amnesia
- Whether the patient has also had manic episodes
- Whether the patient is irrationally afraid of anything
- Whether the patient has experienced difficulty performing familiar tasks
- All of the following are risk factors or diagnostic criteria for Alzheimer’s disease EXCEPT:
- Extra copies of the β-amyloid precursor protein gene.
- Decreased abundance of serotonin and norepinephrine.
- Neurofibrillary tangles of hyperphosphorylated tau protein.
- Deficient blood flow to the parietal lobes.
- Splitting is a defense mechanism commonly seen with which personality disorder?
- Antisocial personality disorder
- Borderline personality disorder
- Histrionic personality disorder
- Narcissistic personality disorder
- A patient comes to the doctor with a two-week history of complete paralysis of the left arm. The patient has had no injury to the extremity, and full neurological workup fails to demonstrate any underlying cause. The patient seems surprisingly unconcerned about the paralysis, and seems more worried about an argument that happened one month ago in which the patient hit a family member. Based on this information, the patient’s most likely diagnosis is:
- conversion disorder.
- generalized anxiety disorder.
- illness anxiety disorder.
- histrionic personality disorder.
- A patient is taken to the doctor after starting to move the fingers in such a way that it looks like rolling something, despite nothing actually being there. The patient also exhibits slowed movement and a shuffling gait. Which neurotransmitter is likely to be present in decreased levels in the patient’s brain?
- Epinephrine
- Histamine
- Dopamine
- Serotonin
- Which of the following is/are true regarding bipolar disorders?
- They have little, if any, genetic heritability.
- They are associated with increased levels of serotonin in the brain.
- They all require at least one depressive episode for diagnosis.
- I only
- II only
- I and III only
- II and III only
Answer Key
- C
- A
- A
- C
- B
- D
- D
- D
- A
- B
- B
- B
- A
- C
- B
Chapter 7: Psychological Disorders
CHAPTER 7
PSYCHOLOGICAL DISORDERS
In This Chapter
7.1 Understanding Psychological Disorders
Biomedical vs. Biopsychosocial Approaches
Classifying Psychological Disorders
Rates of Psychological Disorders
7.2 Types of Psychological Disorders
Schizophrenia
Depressive Disorders
Bipolar and Related Disorders
Anxiety Disorders
Obsessive–Compulsive and Related Disorders
Trauma- and Stressor-Related Disorders
Dissociative Disorders
Somatic Symptom and Related Disorders
Personality Disorders
7.3 Biological Basis of Nervous System Disorders
Schizophrenia
Depressive and Bipolar Disorders
Alzheimer’s Disease
Parkinson’s Disease
Concept Summary
CHAPTER PROFILE
The content in this chapter should be relevant to about 4% of all questions about the behavioral sciences on the MCAT.
This chapter covers material from the following AAMC content category:
7A: Individual influences on behavior
MCAT EXPERTISE
If you’ve taken a glance at the rest of this book, you might have noticed that this chapter has a low percentage of relevant content as compared to the rest of the chapters within MCAT Behavioral Sciences Review. While Chapter 7 materials will be tested less often than the other materials in this book, there are so many psychology questions on the MCAT that even lower-yield topics within the behavioral sciences will get you points!
Introduction
The progress in our understanding of hysteria has come largely through the elaboration of the so-called mechanisms by which the symptoms arise. These mechanisms have been declared to reside or to have their origin in the subconsciousness or coconsciousness. The mechanisms range all the way from the conception of Janet that the personality is disintegrated owing to lowering of the psychical tension to that of Freud, who conceives all hysterical symptoms as a result of dissociation arising through conflicts between repressed sexual desires and experiences and the various censors organized by the social life.
The above is an excerpt from the Journal of Abnormal Psychology in 1915. Merely a century ago, our understanding of psychological disorders was in its infancy. Hysteria—the antiquated name for conversion disorder—was thought to result from marital discord and repressed sexual desires. We are now beginning to understand the underlying psychological and biological factors at play in a number of mental illnesses. In this chapter, we will focus on several different types of psychological disorders, their classification, causes, and frequencies.
7.1 Understanding Psychological Disorders
LEARNING OBJECTIVES
After Chapter 7.1, you will be able to:
- Compare and contrast the biomedical and the biopsychosocial models of psychological disorders
- Recall the most common psychological disorders in the United States
Psychological disorders are characteristic sets of thoughts, feelings, or actions that cause noticeable distress to the sufferer, are considered deviant by the individual’s culture, or cause maladaptive functioning in society, meaning that some aspect of the individual’s behavior negatively impacts others or leads to self-defeating outcomes. Many disorders can be treated once diagnosed. The process of defining these disorders varies, and there are two main classification systems you’ll need to know for the MCAT.
REAL WORLD
Thomas Szasz, an outspoken critic of labeling people “mentally ill,” argues that most of the disorders treated by clinicians are not really illnesses. Rather, they are traits or behaviors that differ from the cultural norm. Szasz argues that labeling people as mentally ill is a way to force them to change and conform to societal norms rather than allowing them to attack the societal causes of their problems.
Biomedical *vs*. Biopsychosocial Approaches
The first classification system to know for the MCAT is the biomedical approach to psychological disorders. Biomedical therapy emphasizes interventions that rally around symptom reduction of psychological disorders. In other words, this approach assumes that any disorder has roots in biomedical disturbances, and thus the solution should also be of a biomedical nature. This view is thought of as narrower than other approaches because it fails to take into account many of the other sources of disorders, such as lifestyle and socioeconomic status. For example, heart disease clearly has roots within the mechanisms of the cardiac muscle, but the causes of these malfunctions have as much to do with biomedical causes (such as genetics) as they do with lifestyle causes (such as a diet rich in salty, fatty foods; smoking; and alcohol use). Similarly, this biomedical approach can miss some underlying sources of psychological disorders and is often more effective when supplemented with a broader approach to diagnosis and treatment.
A broader classification system commonly used for these psychological disorders is the biopsychosocial approach. This method assumes that there are biological, psychological, and social components to an individual’s disorder. The biological component of a disorder is something in the body, like having a particular genetic syndrome. The psychological component of a disorder stems from the individual’s thoughts, emotions, or behaviors. Finally, the disorder’s social component results from the individual’s surroundings and can include issues of perceived class in society and even discrimination or stigmatization. All three of these aspects of a disorder are considered in the biopsychosocial approach for both diagnosis and treatment.
MCAT EXPERTISE
The biopsychosocial model was originally theorized in a 1977 Science article and has grown in breadth, depth, and applicability since it was first described. In fact, the increased recognition of psychological and social factors on patient care was one of the primary drivers for the creation of the Psychological, Social, and Biological Foundations of Behavior section of the MCAT!
To better understand the biopsychosocial approach, consider depression. Certain genetic factors can make an individual more or less susceptible to depressive tendencies, showing a purely biological influence on the disorder. However, from a psychological perspective, the levels of stress that the individual experiences can also contribute to the severity of the depression experienced. Finally, the social environment may provide additional stressors or support from one’s career, family, and friends. Accordingly, in the biopsychosocial model, the goal is often to provide not only direct therapy—treatment that acts directly on the individual, such as medication or periodic meetings with a psychologist—but also indirect therapy, which aims to increase social support by educating and empowering family and friends of the affected individual.
Classifying Psychological Disorders
To aid clinicians in considering these factors, the Diagnostic and Statistical Manual of Mental Disorders (DSM) was created. Originally, the manual was written to collect statistical data in the United States. It is now used as a diagnostic tool in the United States and various other countries. The manual is currently in its fifth edition, which was published in May 2013, so the common abbreviation seen is DSM-5. This manual is a compilation of many known psychological disorders. The DSM-5’s classification scheme is not based on theories of etiology (cause) or treatments of different disorders. Rather, it is based on descriptions of symptoms. It is used by clinicians to fit lists of compiled symptoms from a patient into a category and thus to diagnose that patient. The DSM-5 has 20 diagnostic classes of mental disorders; those that will be tested on the MCAT are discussed in this chapter.
REAL WORLD
David Rosenhan studied whether it was possible to be judged sane if you are in an “insane place” (a psychiatric hospital). Rosenhan and seven other “sane” people were admitted into psychiatric hospitals by reporting auditory hallucinations. Each of these pseudopatients was diagnosed to have either schizophrenia or bipolar disorder, and each was admitted. Once admitted, they acted completely normal—but it still took an average of three weeks to be discharged, and each was still given the diagnosis of schizophrenia in remission. Once labeled, it is very hard to distance oneself from the diagnosis of mental illness.
Rates of Psychological Disorders
Suffering from a mental disorder can be a lonely experience because the disorder usually occurs only in the mind of the patient. However, the rates of these psychological disorders are higher than this experience would otherwise suggest. Table 7.1 covers these rates in detail.
Table 7.1. One-Year Prevalence Rates for Psychological Disorders in the United States
DISORDER PERCENTAGE AFFECTED NUMBER AFFECTED (IN MILLIONS)
Any mental disorder 18.3 44.7
Specific phobia 9.1 22.2
Social anxiety disorder 7.1 17.3
Major depressive disorder 6.7 16.4
Posttraumatic stress disorder 3.6 8.8
Bipolar disorder 2.8 6.8
Generalized anxiety disorder 2.7 6.6
Panic disorder 2.7 6.6
Borderline personality disorder 1.4 3.4
Obsessive–compulsive disorder 1.2 2.9
Agoraphobia 0.9 2.2
Anorexia nervosa 0.6 1.5
Schizophrenia 0.6 1.5
All cancers* 6.1 15.1
Diabetes* 9.4 23.0
*Note: These nonpsychological conditions are included for comparison. All data from this website: https://www.nimh.nih.gov/health/statistics/index.shtml
Treatment of Psychological Disorders
Psychological disorders can be treated in many ways, but treatments fall under the two broad categories of psychopharmacology, or the use of medications, and psychotherapy, or the use of specialized techniques by a trained therapist. Psychotherapy can be further subdivided into talk therapy, which emphasizes verbal interactions and the exploration of thoughts and feelings, and behavioral therapy, which focuses on directly modifying maladaptive behaviors using learning principles.
Examples of talk therapy include psychoanalysis and humanistic therapy (see Chapter 6 for more on the theories of personality these types of therapies are based upon). Behavioral therapy includes techniques like systematic desensitization, a method typically used to treat phobias. In systematic desensitization, a patient with a phobia is gradually exposed to the feared object or situation while being taught relaxation techniques, ultimately reducing the fear response. Some psychotherapies employ a hybrid approach with both talk and behavioral elements, like cognitive behavioral therapy (CBT). CBT, which is one of the most widely practiced types of therapy today, operates on the principle that maladaptive thought patterns and behaviors contribute to psychological distress, and by identifying and modifying these patterns, individuals can experience symptom relief and improved well-being. CBT therapists help individuals challenge negative or distorted thoughts, develop healthier coping mechanisms, and gradually confront feared situations. CBT is used to treat a wide range of disorders, including depression, anxiety disorders, and post-traumatic stress disorder (PTSD).
MCAT EXPERTISE
The MCAT tests many, but not all, categories of mental disorder described within the DSM-5. Neurodevelopmental disorders, eating disorders, impulse control disorders, sleeping disorders, and others are not listed within the AAMC’s guide to MCAT content, and as such are not included within this text.
MCAT CONCEPT CHECK 7.1
Before you move on, assess your understanding of the material with these questions.
- What is the difference between the biomedical and biopsychosocial models of psychological disorders?
____________________________
- Name three psychological disorders with greater than 2% one-year prevalence in the United States (affecting more than 1 in 50 people per year). Refer to Table 7.1 if you get stuck.
- _________________________
- _________________________
- _________________________
7.2 Types of Psychological Disorders
LEARNING OBJECTIVES
After Chapter 7.2, you will be able to:
- List the major positive symptoms and major negative symptoms of schizophrenia and psychotic disorders
- Recall the features of major depressive episodes, manic and hypomanic episodes
- Distinguish between the testable mood disorders
- Relate obsessions and compulsions to the symptoms of obsessive–compulsive disorder
- Describe and explain the symptoms of posttraumatic stress disorder (PTSD)
- Describe and distinguish dissociative and somatic symptom disorders
- Describe the features and individual disorders that fall under cluster A, B, and C personality disorders
As mentioned earlier, the DSM-5 categorizes common symptoms into 20 diagnostic classes. Many of these classes represent significant revisions from the DSM-5’s immediate predecessor, the DSM-IV-TR. The most heavily tested diagnostic classes on the MCAT are schizophrenia spectrum and other psychotic disorders, bipolar and related disorders, depressive disorders, anxiety disorders, obsessive–compulsive and related disorders, trauma- and stressor-related disorders, dissociative disorders, somatic symptom and related disorders, and personality disorders.
Schizophrenia and Other Psychotic Disorders
According to the DSM-5, individuals with a psychotic disorder present with one or more of the following symptoms: delusions, hallucinations, disorganized thought, disorganized behavior, catatonia, and negative symptoms. Like most psychological categories, psychotic disorders are on a spectrum. To delineate the psychotic disorders as described in the DSM-5, psychotic symptoms must be understood.
REAL WORLD
The term schizophrenia is a relatively recent term, coined in 1911 by Eugen Bleuler. Before Bleuler, schizophrenia was called dementia praecox. Schizophrenia literally means “split mind” because the disorder is characterized by distortions of reality and disturbances in the content and form of thought, perception, and affect. Unfortunately, this has led to confusion with dissociative identity disorder (formerly multiple personality disorder). By split mind, Bleuler did not mean that the mind is split into different personalities, but that the mind is split from reality.
Psychotic symptoms are divided into positive and negative types. Positive symptoms are behaviors, thoughts, or feelings added to normal behavior. In other words, positive symptoms are features that are experienced in individuals with psychotic disorders that are not present in the general population. Examples include delusions and hallucinations, disorganized thought, and disorganized or catatonic behavior. Positive symptoms are considered by some to be two distinct dimensions—the psychotic dimension (delusions and hallucinations) and the disorganized dimension (disorganized thought and behavior)—perhaps with different underlying causes. Negative symptoms are those that involve the absence of normal or desired behavior, such as disturbance of affect and avolition.
Positive Symptoms
Delusions are false beliefs discordant with reality and not shared by others in the individual’s culture. These delusions are maintained often in spite of strong evidence to the contrary. Common delusions include delusions of reference, persecution, and grandeur. Delusions of reference involve the belief that common elements in the environment are directed toward the individual. For example, people with delusions of reference may believe that characters in a TV show are talking to them directly. Delusions of persecution involve the belief that the person is being deliberately interfered with, discriminated against, plotted against, or threatened. Delusions of grandeur, also common in bipolar I disorder, involve the belief that the person is remarkable in some significant way, such as being an inventor, historical figure, or religious icon. Other common delusions involve the concept of thought broadcasting, which is the belief that one’s thoughts are broadcast directly from one’s head to the external world, thought withdrawal, the belief that thoughts are being removed from one’s head, and thought insertion, the belief that thoughts are being placed in one’s head.
MCAT EXPERTISE
The fact that delusions must be considered deviant from the society in which an individual lives provides an excellent opportunity for the MCAT to integrate mental illness and sociology. For example, a belief in shamanism—which is common in the Caribbean, Central and South America, Africa, and in some American Indian tribes—would not be considered a delusion within societies that endorse shamanic medicine.
Hallucinations are perceptions that are not due to external stimuli but which nevertheless seem real to the person perceiving them. The most common form of hallucination is auditory, involving voices that are perceived as coming from inside or outside the patient’s head. Visual and tactile hallucinations are less common, but may be seen in drug use or withdrawal.
Disorganized thought is characterized by loosening of associations. This may be exhibited as speech in which ideas shift from one subject to another in such a way that a listener would be unable to follow the train of thought. A patient’s speech may be so disorganized that it seems to have no structure—as though it were just words thrown together incomprehensibly. This is sometimes called word salad. In fact, a person with schizophrenia may even invent new words, called neologisms.
BRIDGE
Word salad can be seen in severe schizophrenia as well as Wernicke’s (receptive) aphasia. Patients will string together unrelated words, although the prosody of the speech (its rhythm, stress, and intonation) remains intact. Aphasias are discussed in Chapter 3 of MCAT Behavioral Sciences Review.
Disorganized behavior refers to an inability to carry out activities of daily living, such as paying bills, maintaining hygiene, and keeping appointments. Catatonia refers to certain motor behaviors characteristic of some people with schizophrenia. The patient’s spontaneous movement and activity may be greatly reduced or the patient may maintain a rigid posture, refusing to be moved. At the other extreme, catatonic behavior may include useless and bizarre movements not caused by any external stimuli, echolalia (repeating another’s words), or echopraxia (imitating another’s actions).
Negative Symptoms
The classic negative symptoms of schizophrenia and related psychotic disorders are disturbance of affect and avolition. Affect refers to the experience and display of emotion, so disturbance of affect is any disruption to these abilities. Affective symptoms may include blunting, in which there is a severe reduction in the intensity of affect expression; emotional flattening (flat affect), in which there are virtually no signs of emotional expression; or inappropriate affect, in which the affect is clearly discordant with the content of the individual’s speech. For example, a patient with inappropriate affect may begin to laugh hysterically while describing a parent’s death. Interestingly, it has become more difficult to assess the affective aspects of schizophrenia because the antipsychotic medications used in treatment frequently blunt and flatten affect as well. Finally, avolition is marked by decreased engagement in purposeful, goal-directed actions.
Schizophrenia
Schizophrenia is the prototypical psychotic disorder in this category of disorders. Schizophrenia is characterized by a break between an individual and reality. In fact, the term schizophrenia literally means “split mind.” Eugen Bleuler coined the term in reference to the splitting of one’s mind from reality. To be given the diagnosis of schizophrenia, an individual must show continuous signs of the disturbance for at least six months, and this six-month period must include at least one month of positive symptoms (delusions, hallucinations, or disorganized speech).
MCAT EXPERTISE
When the MCAT tests schizophrenia, it is likely to include a connection to sociology through the downward drift hypothesis, which states that schizophrenia causes a decline in socioeconomic status, leading to worsening symptoms, which sets up a negative spiral for the patient toward poverty and psychosis. This is why rates of schizophrenia are much, much higher among homeless and indigent people.
Phases of Schizophrenia
The diagnosis and course of schizophrenia typically follows a specific path, termed the phases of schizophrenia. Before schizophrenia is diagnosed, a patient often goes through a phase characterized by poor adjustment. This phase is called the prodromal phase. The prodromal phase is exemplified by clear evidence of deterioration, social withdrawal, role functioning impairment, peculiar behavior, inappropriate affect, and unusual experiences. This is followed by the active phase in which pronounced psychotic symptoms are displayed. If schizophrenia development is slow, correct diagnosis is difficult and the prognosis is especially poor. If the onset of symptoms is intense and sudden, the diagnosis is readily made and the prognosis is better. Diagnosis usually occurs during the active phase. The residual phase, also called the recovery phase, occurs after an active episode and is characterized by mental clarity often resulting in concern or depression as the individual becomes aware of previous behavior.
Other Psychotic Disorders
Other psychotic disorders differ from schizophrenia by the presence, severity, and duration of psychotic symptoms. As a general trend, the other psychotic disorders present symptoms to a lesser degree in comparison to schizophrenia.
- Schizotypal Personality Disorder: Include both personality disorder and psychotic symptoms, with the personality symptoms having been already established before psychotic symptoms present. This condition is covered in greater detail in Personality Disorders.
- Delusion Disorder: Psychotic symptoms are limited to delusions and are present for at least a month.
- Brief Psychotic Disorder: Positive psychotic symptoms are present for at least a day, but less than a month.
- Schizophreniform Disorder: Same diagnostic criteria as schizophrenia except in duration; the required duration for this diagnosis is only 1 month.
- Schizoaffective Disorder: Major mood episodes (major depressive episodes and manic episodes) while also presenting psychotic symptoms.
Depressive Disorders
Sadness is a natural part of life, especially in response to stressful life events like the death of a loved one. During periods of sadness, people might call themselves depressed. However, periodic sadness in response to life events is not a mental disorder. Depressive disorders, in contrast, are conditions characterized by feelings of sadness that are severe enough, in both magnitude and duration, to meet specific diagnostic criteria.
To understand the DSM-5’s categorization of the spectrum of depressive disorders, we must first discuss the 9 depressive symptoms defined in the DSM-5. These symptoms can be recalled with the mnemonic sadness + SIG E. CAPS:
- Sadness: Depressed mood, feelings of sadness and emptiness
- Sleep: Insomnia or hypersomnia
- Interest: Loss of interest and pleasure in activities that previously sparked joy, termed anhedonia
- Guilt: A feeling of inappropriate guilt or worthlessness
- Energy: Lower levels of energy throughout the day
- Concentration: Decrease in ability to concentrate (self described, or observed by others)
- Appetite: Pronounced change in appetite (increase or decrease) resulting in a significant change (5%+) in weight.
- Psychomotor symptoms: Psychomotor retardation (slowed thoughts and physical movements) and psychomotor agitation (restlessness resulting in undesired movement)
- Suicidal thoughts: Recurrent suicidal thoughts
In addition to depressive symptoms, the DSM-5 also categorizes depressive disorders based on duration, timing, and cause of depressive symptoms.
MNEMONIC
Symptoms of a major depressive episode: SIG E. CAPS Sadness +
- Sleep
- Interest
- Guilt
- Energy
- Concentration
- Appetite
- Psychomotor symptoms
- Suicidal thoughts
Major Depressive Disorder
The key diagnostic feature of major depressive disorder (MDD) is the presence of major depressive episodes. A major depressive episode is defined as a 2-week (or longer) period in which 5 of the 9 defined depressive symptoms are encountered, which must include either depressed mood or anhedonia (inability to feel and anticipate pleasure). In addition, the symptoms must be severe enough to impair one’s daily social- or work-related activities.
Persistent Depressive Disorder
Considering the difference in naming between major depressive disorder and persistent depressive disorder, it may seem reasonable to assume that persistent depressive disorder is a lesser form of major depressive disorder. However, this is not the case. In fact, major depressive episodes can coincide with persistent depressive disorder. A diagnosis of persistent depressive disorder (PDD), also known as dysthymia, is given when an individual experiences a period, lasting at least 2 years, in which they experience a depressed mood on the majority of days. With the primary diagnostic feature of PDD being time, a patient can receive both the PDD and MDD diagnosis if they meet both the duration and severity requirements of both disorders.
Other Depressive Disorders
Whereas major depressive disorder and persistent depressive disorder are characterized by severity and duration of depressive symptoms, other depressive disorders can be characterized by their age of incidence and apparent cause.
Children often exhibit more dramatic emotional responses than adults and, in previous editions of the DSM, this led to the potential overdiagnosis of bipolar disorders in children. To address this concern the DSM-5 includes disruptive mood dysregulation disorder, which is typically diagnosed between the ages of 6 and 10, and has the key diagnostic feature of persistent and recurrent emotional irritability in multiple environments (school, home, etc.).
Depressive symptoms can also arise in response to specific times and situations; if these symptoms meet certain diagnostic criteria then they are considered disorders. Premenstrual dysphoric disorder is characterized by mood changes, often depressed mood, occurring a few days before menses and resolving after menses onset.
Although not freestanding diagnoses in the DSM-5, both seasonal affective disorder and postpartum depression are conditions that have an apparent cause. In seasonal affective disorder (SAD), the dark winter months are believed to be the source of depressive symptoms and thus the disorder is best categorized as major depressive disorder with seasonal onset, while in postpartum depression the rapid change in hormone levels just after giving birth is the cause of the depressive symptoms. In the case of seasonal affective disorder, depressive symptoms are present only in the winter months. This disorder may be related to abnormal melatonin metabolism; it is often treated with bright light therapy, where the patient is exposed to a bright light for a specified amount of time each day, as demonstrated with a plant in Figure 7.1.

Figure 7.1. Bright Light Therapy for Seasonal Affective Disorder
BRIDGE
The most common first-line treatment for depression is the class of medications called selective serotonin reuptake inhibitors (SSRIs). These block the reuptake of serotonin by the presynaptic neuron, resulting in higher levels of serotonin in the synapse and relief of symptoms. The nervous system is outlined in Chapter 1 of MCAT Behavioral Sciences Review and Chapter 4 of MCAT Biology Review.
Bipolar and Related Disorders
This category of disorders is characterized by the presence of manic and depressive symptoms, which if severe and persistent enough can be labelled as episodes. Manic symptoms are associated with an exaggerated elevation in mood, accompanied by an increase in goal-directed activity and energy. Put simply, manic symptoms can be thought of as the prolonged and exaggerated emotion of happiness or joy. According to the DSM-5, there are 7 manic symptoms. These symptoms can be recalled with the mnemonic DIG FAST:
- Distractibility: Inability to remain focused on an activity
- Irresponsibility: Engaging in risky activities without considering future consequences
- Grandiosity: Exaggerated and unrealistic increase in self-esteem
- Flight of thoughts: Racing thoughts, self-reported or revealed through rapid speech
- Activity or agitation: Increase in goal-oriented work or social activities
- Sleep: Decreased need for sleep, e.g. sleeping for only a couple hours but feeling rested
- Talkative: Exaggerated desire to speak
The presence of manic symptoms are considered a hypomanic episode if the symptoms are present for at least 4 days and include at least 3 or more of the 7 defined manic symptoms, yet the symptoms are not severe enough to impair the person’s social or work activities. However, the diagnosis progresses to a manic episode if the manic symptoms (3 or more of the defined 7) are severe enough to impair a person’s social or work activities and persist for at least 7 days.
In addition to manic symptoms and their associated episodes, the presence or absence of depressive symptoms and their associated episodes are also used to differentiate bipolar and related disorders. Specifically, these disorders are classified by the presence or absence of manic, hypomanic, and major depressive episodes. Depressive symptoms were covered in Depressive Disorders.
Bipolar I Disorder
When manic episodes are present, a diagnosis of bipolar I disorder is likely to be made, as the key diagnostic feature of this disorder is the presence of manic episodes. While most diagnoses of bipolar I disorder also include depressive symptoms, often major depressive episodes, they are not a requirement. To illustrate this point consider two hypothetical patients: Patient A only experiences manic episodes, while Patient B regularly experiences both manic and major depressive episodes, cycling between the two regularly. Despite both patients presenting very differently, both fit the categorization of bipolar I disorder.
Bipolar II Disorder
The key feature of a bipolar II disorder diagnosis is the presence of both a major depressive episode and an accompanying hypomanic episode, but not a manic episode. To avoid confusion, it is worth noting that if a patient has experienced both major depressive episodes and manic episodes, a diagnosis of bipolar I disorder will likely be made. In addition, if a person experiences only major depressive symptoms (absence of hypomanic and manic episodes), then a diagnosis of major depressive disorder is likely to be made. Thus, the diagnosis of bipolar II only captures individuals who experience major depressive episodes and the lesser, hypomanic episodes.
Cyclothymic Disorder
The diagnostic features of cyclothymic disorder are the presence of both manic and depressive symptoms that are not severe enough to be considered episodes. In other words, the patient has not experienced major depressive, manic, or hypomanic episodes. Or, more specifically, the patient has never experienced 3 or more of the 7 manic symptoms in a 4 day period (diagnostic criteria for hypomanic episode) and has never experienced 5 or more of the 9 depressive symptoms in a 2-week period (diagnostic criteria for a major depressive episode). Considering the relatively low threshold of symptom requirements, it may seem that everyone would be diagnosed with cyclothymic disorder. However despite the relatively low symptom requirements, the duration requirements for this disorder are high. For a diagnosis of cyclothymic disorder to be made, a person must have experienced numerous periods of manic and depressive symptoms for the majority of time over a 2-year (or longer) period.
Before moving on to anxiety disorders, a brief discussion of proposed neurological etiologies of mood disorders is warranted. The most common explanation revolves around the neurotransmitters norepinephrine and serotonin. These two are often linked together into what is called the monoamine or catecholamine theory of depression. This theory holds that too much norepinephrine and serotonin in the synapse leads to mania, while too little leads to depression. Although more recent research has shown that it is not that simple, you should be aware of this theory for the MCAT.
REAL WORLD
Depressive and manic episodes are essentially two sides of the same coin: Depression is associated with low norepinephrine and serotonin levels, and manic episodes are associated with high levels of these neurotransmitters. When patients are put on treatment for depression, they must be watched for signs of mania because antidepressant medications may trigger manic symptoms or episodes.
Anxiety Disorders
From an evolutionary perspective, emotions served to direct and modulate behavior based on environmental stimuli. As seen in bipolar and depressive disorders, when the regulation of emotions, such as happiness or sadness, are insufficient, then symptoms arise. In the case of anxiety, fear is the associated emotion. Fear is often defined as an emotional response to an immediate threat, while anxiety can be viewed as fear of an upcoming or future event. Like fear, anxiety is healthy and important in one’s life. It is only considered an anxiety disorder when irrational and excessive fear or anxiety affects an individual’s daily functioning.
There are more than 10 disorders listed in the anxiety disorders portion of the DSM-5. These disorders are categorized by the situation or stimulus that induces anxiety.
BRIDGE
For all anxiety disorders, clinicians must rule out hyperthyroidism—excessive levels of the thyroid hormones triiodothyronine (T3) and thyroxine (T4)—because increasing the whole body’s metabolic rate will create anxiety-like symptoms. Thyroid function is discussed in Chapter 5 of MCAT Biology Review.
Specific Phobias
The most common type of anxiety disorder is a phobia. A phobia is an irrational fear of something that results in a compelling desire to avoid it. Most of the phobias that you are likely familiar with are what the DSM-5 calls specific phobias. A specific phobia is one in which fear and anxiety are produced by a specific object or situation. Unlike other sources of anxiety, specific phobias lack a specific ideation or thought pattern and instead present as an immediate and irrational fear response to the specific object or situation. For example, claustrophobia is an irrational fear of closed places, acrophobia is an irrational fear of heights, and arachnophobia is an irrational fear of spiders.

Figure 7.2. Specific Phobia Arachnophobia, the fear of spiders, is a common example of a specific phobia.
Separation Anxiety Disorder
Separation anxiety is the excessive fear of being separated from one’s caregivers or home environment. Although some separation anxiety is common and to be expected in young children, when this anxiety is excessive and persists beyond the age where it is deemed developmentally appropriate, the person may be diagnosed with separation anxiety disorder. This diagnosis is accompanied by the ideation that when separated, the caregiver or the individual themselves will be harmed (e.g. kidnapping, getting sick). These persistent beliefs may result in avoidant behaviors such as refusal to leave the home, shadowing the caregiver, etc.
Social Anxiety Disorder
On the surface, social anxiety disorder can be viewed as a social phobia, that is, fear and anxiety towards social situations and encounters. However, unlike previously discussed specified phobias, social anxiety disorder has an accompanying ideation in which individuals think that they will be perceived negatively by others. Thus, the key diagnostic feature of social anxiety disorder is fear or anxiety towards social situations with the belief that the individual will be exposed, embarrassed, or simply negatively perceived by others.
Like other anxiety disorders, avoidant behaviors are often conditioned as a means to reduce the associated anxiety. In the case of social anxiety, this can be as broad as avoiding social situations entirely or as narrow as avoiding handshakes out of fear of sweaty palms. Avoidant behavior to the point of social or occupational impairment is necessary for a social anxiety disorder diagnosis.
Selective Mutism
Although categorized as a separate anxiety disorder, selective mutism is heavily associated with social anxiety disorder and characterized by the consistent inability to speak in situations where speaking is expected. However, in situations that are more relaxed or when communication is not expected, speaking is unaffected. From this perspective, selective mutism may be conceptualized as a patient’s fear of being negatively evaluated for what the patient might say.
Panic Disorder
The key diagnostic feature of panic disorder is the recurrence of unexpected panic attacks. To understand panic disorder, we must first cover panic attacks. From a physiological perspective, a panic attack is the misfiring of the sympathetic nervous system resulting in an unwanted fight or flight response. From a psychological perspective, a panic attack includes the associated emotions that accompany the sympathetic response, such as intense fear and a sense of impending doom/danger. Combining these two perspectives, a panic attack is the sudden surge of fear in which individuals feel that they are losing control of their body and/or that they are dying. The occurrence of an individual’s attacks may be associated with specific triggers, in which case the attacks are termed expected panic attacks. If there is no clear trigger and the panic attacks are seemingly random, they are termed unexpected panic attacks.
The diagnosis of panic disorder requires the recurrence of unexpected panic attacks. The unexpected panic attacks themselves can produce an associated anxiety. In other words, an individual may become anxious at the thought of having an unexpected panic attack. If this anxiety impairs one’s daily functions and persists for at least a month, then the diagnosis of panic disorder is made.
It is worth noting that panic attacks themselves are not considered a psychological disorder. They may occur in the absence of physiological disorders or may be associated with anxiety disorders in which there is a clear trigger. For instance, an individual with arachnophobia may experience expected panic attacks when encountering a spider.
BRIDGE
Notice that a large number of the symptoms of panic disorder are caused by excess activation of the sympathetic nervous system (autonomic overdrive). These include trembling, sweating, hyperventilation, shortness of breath, a racing heart rate, and palpitations. The autonomic nervous system is discussed in Chapter 1 of MCAT Behavioral Sciences Review and Chapter 4 of MCAT Biology Review.
Agoraphobia
Agoraphobia is an anxiety disorder characterized by a fear of being in places or situations where it might be difficult for an individual to escape. This fear may stem from the thought that the individual may experience a panic attack or similar event in which they would need to escape to avoid embarrassment. People who have agoraphobia tend to be uncomfortable leaving their homes, using public transport, being in open spaces, waiting in lines, or simply being in crowds. Due to agoraphobia’s association with panic attacks and fear of being negatively evaluated by others, it is often comorbid with panic disorder, social anxiety disorder, and specific phobias.
Generalized Anxiety Disorder
As previously mentioned, the DSM-5 categorizes anxiety disorders based on the stimulus that induces fear or anxiety. For instance, anxiety towards social interactions is termed social anxiety; anxiety at the thought of separation from one’s caregivers is termed separation anxiety. On the other hand, some individuals have more anxious temperaments, making them susceptible to anxiety triggered by a multitude of stimuli. It is for this reason that specific anxiety disorders are often comorbid with one another, resulting in patients having multiple diagnoses. However, a better diagnosis for some patients with many triggers for anxiety might be generalized anxiety disorder.
Generalized anxiety disorder (GAD) is defined as a disproportionate and persistent worry about many different things—making mortgage payments, doing a good job at work, returning emails, political issues, and so on—for at least six months. In addition, the worrying is difficult to control, even in cases where the individual knows that their worrying and fear is irrational. These individuals often have physical symptoms like fatigue, muscle tension, and sleep problems that accompany the worry. General anxiety disorder is relatively common in the US population, with approximately 3% of the population experiencing GAD in a 12-month period. Furthermore, over the course of a lifetime, individuals have a 1 in 10 chance of meeting the diagnostic criteria for general anxiety disorder.
Obsessive–Compulsive and Related Disorders
Formerly classified under anxiety and somatic symptom disorders, the disorders in this group were relabeled as obsessive–compulsive and related disorders in the DSM-5. The reason for this organizational change reveals the common feature among these conditions. Across all of the following disorders, individuals perceive a particular need and respond to the need by completing a particular action. Disorders in this category are differentiated by the compulsiveness of the need to be met as well as the nature of the action.
Obsessive–Compulsive Disorder
Obsessive–compulsive disorder (OCD) is characterized by obsessions (persistent, intrusive thoughts and impulses), which produce tension, and compulsions (repetitive tasks) that relieve tension but cause significant impairment in a person’s life. The relationship between the two is key: obsessions raise the individual’s stress level, and the compulsions relieve this stress. Obsessions and their compulsions are ego-dystonic, meaning that the individual knows that their behavior is irrational, but the anxiety that arises when compulsions are not performed cannot be ignored.
Obsessions are perceived needs with the accompanying ideation that if a particular need is not met, then disastrous events will follow. Actions paired with obsessions are termed compulsions. As individuals with OCD attempt to satisfy their obsessions, rituals or sets of rules are developed for how their compulsions must be performed. For example, individuals may need to wash their hands for a specific length of time or else the intrusive thought of getting sick occurs. Alternatively, individuals may need to check if their door is locked a specific number of times or else worry obsessively about getting robbed. To be diagnosed with OCD, the compulsions must impair one’s daily activities, for instance by taking up a lot of time during the day.
Body Dysmorphic Disorder
In body dysmorphic disorder, a person has an unrealistic negative evaluation of personal appearance and attractiveness, usually directed toward a certain body part. This is known as a preoccupation, a type of worry which lacks the disastrous ideation that accompanies obsessions. Patients with this disorder see their nose, skin, or stomach as ugly or even horrific when actually ordinary in appearance. This body–focused preoccupation also disrupts day-to-day life, and the sufferer may seek multiple plastic surgeries or other extreme interventions. A common association with this disorder is muscle dysmorphia, in which individuals believe that their body is too small or unmuscular (a preoccupation) and respond through working out. Like body dysmorphic disorder in general, this belief persists even with clear evidence to the contrary.
Hoarding Disorder
Hoarding disorder presents as a need to save or keep items and is often paired with excessive acquisition of objects. This behavior stems from several possible sources, ranging from the belief that kept items will eventually be useful to the feeling that the patient has a responsibility to care for the items. As a result, individuals with hoarding disorder often fill their homes with seemingly useless items even past the point where the accumulation of belongings impairs daily life.
Obsessive–Compulsive and Related Disorders with Body-Focused Repetitive Behaviors
Trichotillomania and excoriation are two obsessive–compulsive and related disorders that both present with body-focused compulsions. In the case of trichotillomania, individuals are compelled to pull out their hair, while with excoriation disorder, individuals are compelled to pick at their skin. A required diagnostic feature in both of these disorders is that patients have previously attempted to stop their body-focused compulsions but have so far failed.
Trauma- and Stressor-Related Disorders
This category captures disorders where a traumatic event is the source of the symptoms and thus is a diagnostic requirement in these disorders. The typical response to traumatic events includes fear, helplessness, and perhaps anxiety. In trauma and stressor related disorders, however, individuals also present with maladaptive symptoms like anhedonia, dysphoria (generalized dissatisfaction with life), aggression, or dissociation.
By far, the most notable disorder in this category is posttraumatic stress disorder (PTSD). PTSD occurs after experiencing or witnessing a traumatic event, such as war, a home invasion, rape, or a natural disaster, and consists of intrusion symptoms, arousal symptoms, avoidance symptoms, and negative cognitive symptoms.
- Intrusion symptoms include recurrent reliving of the event, flashbacks, nightmares, and prolonged distress.
- Arousal symptoms include an increased startle response, irritability, anxiety, self-destructive or reckless behavior, and sleep disturbances.
- Avoidance symptoms include deliberate attempts to avoid the memories, people, places, activities, and objects associated with the trauma.
- Negative cognitive symptoms include an inability to recall key features of the event, negative mood or emotions, feeling distanced from others, and a persistent negative view of the world.
To meet the criteria of PTSD, a particular number of these symptoms must be present for at least one month. If the same symptoms last for less than one month (but more than three days), it may be called acute stress disorder.
From a behaviorist perspective, symptoms of PTSD can be explained by the traumatic event and one’s reaction to it. Intrusion and arousal symptoms can be explained by associative learning, specifically classical conditioning, in which the event has become associated with traumatic triggers and has generalized to include everyday stimuli. Avoidance symptoms can be explained through operant conditioning, specifically avoidance learning, in which an individual learns behavior to avoid unpleasant stimuli, or involuntary responses in the case of PTSD. Finally, negative cognitive symptoms can be viewed as a form of dissociation, which is a defense mechanism to avoid unpleasant stimuli. Dissociation will be covered in greater detail in Dissociative Disorders.
Dissociative Disorders
Patients with dissociative disorders avoid stress by escaping from parts of their identity. Such patients otherwise still have an intact sense of reality. Examples of dissociative disorders include dissociative amnesia, dissociative identity disorder (formerly multiple personality disorder), and depersonalization/derealization disorder.
Dissociative Amnesia
Dissociative amnesia is characterized by an inability to recall past experiences. The qualifier dissociative simply means that the amnesia is not due to a neurological disorder. This disorder is often linked to trauma. Some individuals with this disorder may also experience dissociative fugue: a sudden, unexpected move or purposeless wandering away from one’s home or location of usual daily activities. Individuals in a fugue state are confused about their identity and can even assume a new identity. Significantly, they may actually believe that they are someone else, with a complete backstory.
Dissociative Identity Disorder
In dissociative identity disorder (DID, formerly multiple personality disorder), there are two or more personalities that recurrently take control of the patient’s behavior, as represented in Figure 7.3. This disorder results when the components of identity fail to integrate. In most cases, patients have suffered severe physical or sexual abuse as young children. After much therapy, the personalities can sometimes be integrated into one. The existence of dissociative identity disorder is justifiably debated within the medical community, but its characteristics are still important to recognize on Test Day.

Figure 7.3. Dissociative Identity Disorder (DID) One artist’s interpretation of many personalities seen in DID.
REAL WORLD
One of the first and most famous cases of dissociative identity disorder in the media is Shirley Ardell Mason, also known as “Sybil,” who claimed to have at least 13 separate personalities. Mason underwent years of therapy in an attempt to combine her personalities into a single one. Two separate TV movies, both called Sybil, have been produced to tell the story of Sybil’s struggle with this disorder.
Depersonalization/Derealization Disorder
In depersonalization/derealization disorder, individuals feel detached from their own minds and bodies (depersonalization) or from their surroundings (derealization). This often presents as a feeling of automation, and can include symptoms like a failure to recognize one’s reflection. An out-of-body experience is an example of depersonalization. Derealization is often described as giving the world a dreamlike or insubstantial quality. Such patients may also experience depersonalization and derealization simultaneously. These feelings cause significant impairment of regular activities. However, even during these times, such patients do not display psychotic symptoms like delusions or hallucinations.
Somatic Symptom and Related Disorders
Diagnoses in this category are marked by somatic (bodily) symptoms that cause significant stress or impairment.
Somatic Symptom Disorder
Individuals with somatic symptom disorder have at least one somatic symptom, which may or may not be linked to an underlying medical condition, and that is accompanied by disproportionate concerns about its seriousness, devotion of an excessive amount of time and energy to it, or elevated levels of anxiety.
Illness Anxiety Disorder
Illness anxiety disorder is characterized by being consumed with thoughts about having or developing a serious medical condition. Individuals with this disorder are quick to become alarmed about their health, and either excessively check themselves for signs of illness or avoid medical appointments altogether. Most patients classified under hypochondriasis in the DSM-IV-TR now fit into either somatic symptom disorder if somatic symptoms are present, or illness anxiety disorder if they are not.
Conversion Disorder
Conversion disorder, also known as functional neurological symptom disorder, is characterized by symptoms affecting voluntary motor or sensory functions that are incompatible with the patient’s neurophysiological condition. The symptoms generally begin soon after the individual experiences high levels of stress or a traumatic event, but may not develop until some time has passed after the initiating experience. Examples include paralysis or blindness without evidence of neurological damage. The patient may be surprisingly unconcerned by the symptom—what is called la belle indifférence. Conversion disorder was historically called hysteria. The symptoms seen in conversion disorder may sometimes be connected with the inciting event in a literal or poetic way; for example, a parent going blind shortly after watching a child die tragically.
Personality Disorders
A personality disorder is a pattern of behavior that is inflexible and maladaptive, causing distress or impaired functioning in at least two of the following: cognition, emotions, interpersonal functioning, or impulse control. Personality disorders are considered ego-syntonic, meaning that individuals perceive their behavior as correct, normal, or in harmony with their goals. This is in contrast to the other disorders covered in this chapter that are ego-dystonic, meaning that individuals see the illness as something thrust upon them that is intrusive and bothersome. In addition to general personality disorder (which fits the diagnostic criteria described above), there are ten personality disorders grouped into three clusters: cluster A (paranoid, schizotypal, and schizoid), cluster B (antisocial, borderline, histrionic, and narcissistic), and cluster C (avoidant, dependent, and obsessive–compulsive). Personality disorder criteria will continue changing over time; the DSM-5 includes a section specifically devoted to research models for redefining personality disorders.
REAL WORLD
The distinction between ego-syntonic and ego-dystonic symptoms is a key feature in differential diagnosis of disorders in the DSM-5. For instance, social anxiety disorder shares many of the same symptoms as avoidant personality disorder, such as anxiety directed towards social interactions and maladaptive avoidance behavior. The distinction between these disorders is that individuals with social anxiety disorder often know that their fear of being ridiculed is irrational (ego-dystonic), while individuals with avoidant personality disorder actually believe they are inferior and that their fear of ridicule is valid (ego-syntonic).
Cluster A (Paranoid, Schizotypal, and Schizoid Personality Disorders)
The cluster A personality disorders are all marked by behavior that is labeled as odd or eccentric by others. Its three examples include paranoid, schizotypal, and schizoid personality disorders.
Paranoid personality disorder is marked by a pervasive distrust of others and suspicion regarding their motives. In some cases, these patients may actually be in the prodromal phase of schizophrenia and are termed premorbid.
Schizotypal personality disorder refers to a pattern of odd or eccentric thinking. These individuals may have ideas of reference (similar to delusions of reference, but not as extreme in intensity) as well as magical thinking, such as superstitiousness or a belief in clairvoyance.
Finally, schizoid personality disorder is a pervasive pattern of detachment from social relationships and a restricted range of emotional expression. People with this disorder show little desire for social interactions, have few or no close friends, and have poor social skills. It should be noted that neither schizotypal nor schizoid personality disorder are the same as schizophrenia.
Cluster B (Antisocial, Borderline, Histrionic, and Narcissistic Personality Disorders)
The cluster B personality disorders are all marked by behavior that is labeled as dramatic, emotional, or erratic by others. Its four examples include antisocial, borderline, histrionic, and narcissistic personality disorders.
Antisocial personality disorder is three times more common in males than in females. The essential feature of the disorder is a pattern of disregard for and violations of the rights of others. This is evidenced by repeated illegal acts, deceitfulness, aggressiveness, or a lack of remorse for said actions. Many serial killers and career criminals who show no guilt for their actions have this disorder. Additionally, people with this disorder comprise about 20 to 40 percent of prison populations.
Borderline personality disorder is two times more common in females than in males. In this disorder, there is pervasive instability in interpersonal behavior, mood, and self-image. Interpersonal relationships are often intense and unstable. There may be profound identity disturbance with uncertainty about self-image, sexual identity, long-term goals, or values. There is often intense fear of abandonment. Individuals with borderline personality disorder may use splitting as a defense mechanism, in which they view others as either all good or all bad (an angel vs. devil mentality). Suicide attempts and self-mutilation (cutting or burning) are common.
Histrionic personality disorder is characterized by constant attention-seeking behavior. These individuals often wear colorful clothing, are dramatic, and are exceptionally extroverted. They may also use seductive behavior to gain attention.
In narcissistic personality disorder, the patient has a grandiose sense of self-importance or uniqueness, preoccupation with fantasies of success, a need for constant admiration and attention, and characteristic disturbances in interpersonal relationships such as feelings of entitlement. As used in everyday language, narcissism refers to those who like themselves too much. However, people with narcissistic personality disorder have very fragile self-esteem and are constantly concerned with how others view them. There may be marked feelings of rage, inferiority, shame, humiliation, or emptiness when these individuals are not viewed favorably by others.
Cluster C (Avoidant, Dependent, and Obsessive–Compulsive Personality Disorders)
The cluster C personality disorders are all marked by behavior that is labeled as anxious or fearful by others. Its three examples include avoidant, dependent, and obsessive–compulsive personality disorders.
In avoidant personality disorder, the affected individual has extreme shyness and fear of rejection. Individuals who have this disorder will see themselves as socially inept and are often socially isolated, despite an intense desire for social affection and acceptance. These individuals tend to stay in the same jobs, life situations, and relationships despite wanting to change.
Dependent personality disorder is characterized by a continuous need for reassurance. Individuals with dependent personality disorder tend to remain dependent on one specific person, such as a caregiver or significant other, to take actions and make decisions.
In obsessive–compulsive personality disorder (OCPD), the individual is perfectionistic and inflexible, tending to like rules and order. Other characteristics may include an inability to discard worn-out objects, lack of desire to change, excessive stubbornness, lack of a sense of humor, and maintenance of careful routines. Note that obsessive–compulsive personality disorder is not the same as obsessive–compulsive disorder. Whereas OCD has obsessions and compulsions that are focal and acquired, OCPD is lifelong. OCD is also ego-dystonic (I can’t stop washing my hands because of the germs!), whereas OCPD is ego-syntonic (I just like rules and order!).
BEHAVIORAL SCIENCES GUIDED EXAMPLE WITH EXPERT THINKING
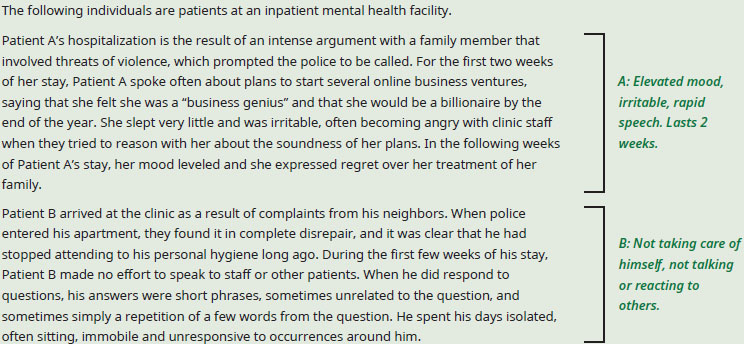
Based only on the information provided, what diagnosis from the DSM-5 is most likely for each of these patients?
If you’re asked to make a diagnosis for a hypothetical patient, make a checklist of the symptoms described in the passage or question, and then match them to what you know about the disorders that are within the scope of the MCAT. It is worth taking a moment to consider the severity of the symptoms as well, since it can help to differentiate between similar disorders (depression and dysthymic disorder, for example).
Patient A exhibits grandiose self-esteem, rapid speech, a lack of need for sleep, and irritability, which are all symptoms of mania and together are sufficient to apply the label of manic episode. The described transition out of mania into a different mood state suggests bipolar disorder. Specifically, the presence of a full manic episode rules out bipolar II and would lead to a diagnosis of bipolar I, which does not require a depressive episode to follow.
Patient B is trickier, but consider that the writers of the MCAT know that you are not a trained psychiatrist and so will not require a nuanced diagnosis from you. The symptoms that they present will be straightforward and should add up to a description of a disorder that you are familiar with. For patient B, those symptoms are avolition (an inability to perform basic goal-directed activities), flat or blunted affect (lack of emotional expression), and alogia (reduction in speaking). These are all negative symptoms of schizophrenia. The description of patient B also includes echolalia (repetition of words or short phrases), which is a positive symptom and is a signal to you as a test taker that this is indeed schizophrenia, rather than a case of severe depression. While there is still the possibility that Patient B has another, related disorder, the MCAT would not present you with a choice that would require you to distinguish between, say, schizophrenia and schizoid personality disorder without substantial additional information allowing that decision to be made.
In summary, patient A is most likely experiencing bipolar I disorder, and patient B is most likely experiencing schizophrenia or a related disorder.
KEY CONCEPT
Obsessive–compulsive disorder (OCD) and obsessive–compulsive personality disorder (OCPD) are not synonymous. OCD is marked by obsessions (intrusive thoughts causing tension) and compulsions (repetitive tasks that relieve this tension but cause significant impairment). OCPD is a personality disorder in which individuals are perfectionistic and inflexible.
MCAT CONCEPT CHECK 7.2
Before you move on, assess your understanding of the material with these questions.
- A schizophrenic patient is started on the atypical antipsychotic risperidone, which is effective for treatment of the positive symptoms of schizophrenia, but not the negative symptoms. Which of the patient’s symptoms are likely to improve, and which are not? _________________________
- What are the features of a major depressive episode? Of a manic episode?
____________________________
- Major depressive episode:
____________________________
- Manic episode:
- For each of the following disorders, briefly describe their makeup with respect to depressive episodes, manic episodes, and other mood disturbances:
____________________________
- Major depressive disorder:
____________________________
- Bipolar I disorder:
____________________________
- Bipolar II disorder:
_________________________
- Cyclothymic disorder:
- A patient with obsessive–compulsive disorder believes that the latch on the apartment door must be checked five times before it is okay to go to bed. Without checking the latch five times, the patient cannot sleep for fear that someone will break into the apartment. Identify the patient’s obsession, the patient’s compulsion, and how they are related in obsessive–compulsive disorder.
____________________________
- Obsession:
____________________________
- Compulsion:
____________________________
- Relationship:
- What features describe each cluster of personality disorders? Which personality disorders fall into each cluster?
Cluster Features Personality Disorders A B C
7.3 Biological Basis of Nervous System Disorders
LEARNING OBJECTIVES
After Chapter 7.3, you will be able to:
- Describe the impact of depression on hormone and neurotransmitter levels
- Recall the general features and risk factors for Alzheimer’s disease
- Explain the role of dopamine in schizophrenia and Parkinson’s disease
In addition to knowing the psychological and sociological components of these diagnoses, the MCAT also expects you to know the biological basis of a few mental disorders. These disorders include schizophrenia, depression, Alzheimer’s disease, and Parkinson’s disease. Research into how to stop the progression of the biological component of these diseases is widespread and will also be something to stay apprised of as a medical student and a physician.
Schizophrenia
Schizophrenia is an area of active research, though some biological factors have been isolated. Most potential causes are genetic, but trauma at birth, especially hypoxemia (low oxygen concentrations in the blood), is also considered to be a risk factor. Other exposures may also play a role; excessive marijuana use in adolescence is associated with increased risk. There is significant data to indicate that schizophrenia is partially inherited. If a person has this disorder, the risk that first-degree relatives will also have the disorder is ten times that of an unrelated person in the general population; this measurement controls for environmental effects.
Schizophrenia may be associated with structural changes in the brain, but more research is needed to determine their significance and prevalence within the affected population. Schizophrenia is highly associated with an excess of dopamine in the brain; many medications used to treat schizophrenia, such as neuroleptics, block dopamine receptors. The term neuroleptic means that these medications depress nerve function. Neuroleptics are also known as antipsychotics.
Depressive and Bipolar Disorders
There are a host of markers associated with depression:
- Abnormally high glucose metabolism in the amygdala
- Hippocampal atrophy after a long duration of illness
- Abnormally high levels of glucocorticoids (cortisol)
- Decreased norepinephrine, serotonin, and dopamine (monoamine theory of depression)
It has been found that both these neurotransmitters and their metabolites are decreased in depressed patients, meaning that their actual production is decreased (rather than production staying the same and their degradation increasing).
For bipolar disorders, there exists a different set of biological factors and genetic corollaries that contribute to the disease:
- Increased norepinephrine and serotonin (monoamine theory)
- Higher risk if parent has bipolar disorder
- Higher risk for persons with multiple sclerosis
Alzheimer’s Disease
Alzheimer’s disease is a type of dementia characterized by gradual memory loss, disorientation to time and place, problems with abstract thought, and a tendency to misplace things. Later stages of the disease are associated with changes in mood or behavior, changes in personality, difficulty with procedural memory, poor judgment, and loss of initiative. Now, each of these symptoms alone doesn’t necessarily point to Alzheimer’s; however, when all or almost all of these symptoms are seen in one person, and especially when the symptoms end up inhibiting normal daily function, this points to Alzheimer’s disease. This disease is most common in patients older than 65, and women are at greater risk than men. Family history is a significant risk factor and, interestingly, there is a lower risk of developing the disease with higher levels of education.
There is a genetic component to Alzheimer’s disease. Research shows that mutations in the presenilin genes on chromosomes 1 and 14 contribute to having the disease, and mutations in the apolipoprotein E gene on chromosome 19 can also alter the likelihood of acquiring the disease. Finally, the β-amyloid precursor protein gene on chromosome 21 is known to contribute to Alzheimer’s disease, explaining the much higher risk of Alzheimer’s in individuals with Down syndrome.
While the precise biological cause of Alzheimer’s disease is unknown, there are many biological markers that are found in patients with the disease. Don’t worry about understanding each of these markers in depth, but rather be able to recognize these factors if you see them on the MCAT:
- Diffuse atrophy of the brain on CT or MRI
- Flattened sulci in the cerebral cortex
- Enlarged cerebral ventricles, shown in Figure 7.4(a)
- Deficient blood flow in parietal lobes, which is correlated with cognitive decline
- Reduction in levels of acetylcholine
- Reduction in choline acetyltransferase (ChAT), the enzyme that produces acetylcholine
- Reduced metabolism in temporal and parietal lobes
- Senile plaques of ***β*-amyloid** (a misfolded protein in β-pleated sheet form), shown in Figure 7.4(b)
- Neurofibrillary tangles of hyperphosphorylated tau protein, shown in Figure 7.4(c)

Figure 7.4(a). Symptoms of Alzheimer’s Disease Enlarged cerebral ventricles (left) vs. normal cerebral ventricles (right)
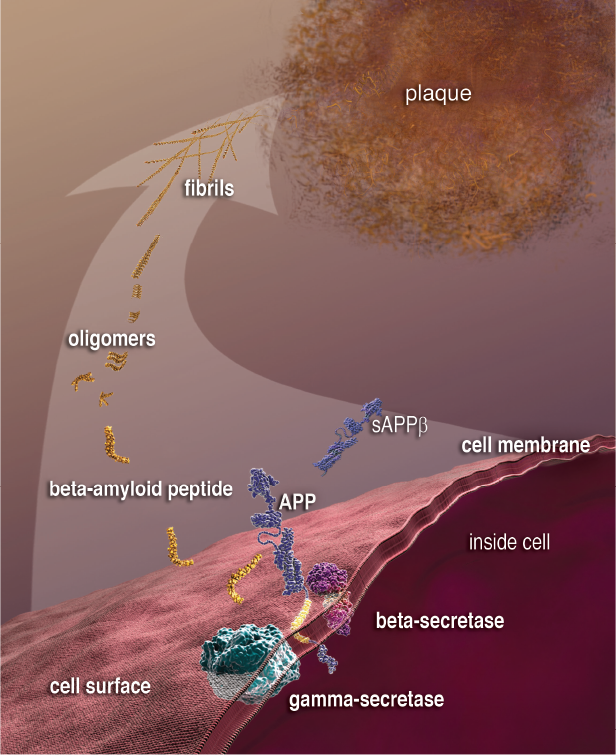
Figure 7.4(b). Symptoms of Alzheimer’s Disease Formation of senile plaques ofβ-amyloid

Figure 7.4(c). Symptoms of Alzheimer’s Disease Neurofibrillary tangles of hyperphosphorylated tau protein (magenta)
Parkinson’s Disease
Parkinson’s disease, demonstrated in Figure 7.5, is characterized by bradykinesia (slowness in movement), resting tremor (a tremor that appears when muscles are not being used), pill-rolling tremor (flexing and extending the fingers while moving the thumb back and forth, as if rolling something in the fingers), masklike facies (static and expressionless facial features, staring eyes, and a partially open mouth), cogwheel rigidity (muscle tension that intermittently halts movement as an examiner attempts to manipulate a limb), and a shuffling gait with stooped posture. A common but not characteristic symptom is depression. Dementia is also common in Parkinson’s disease.
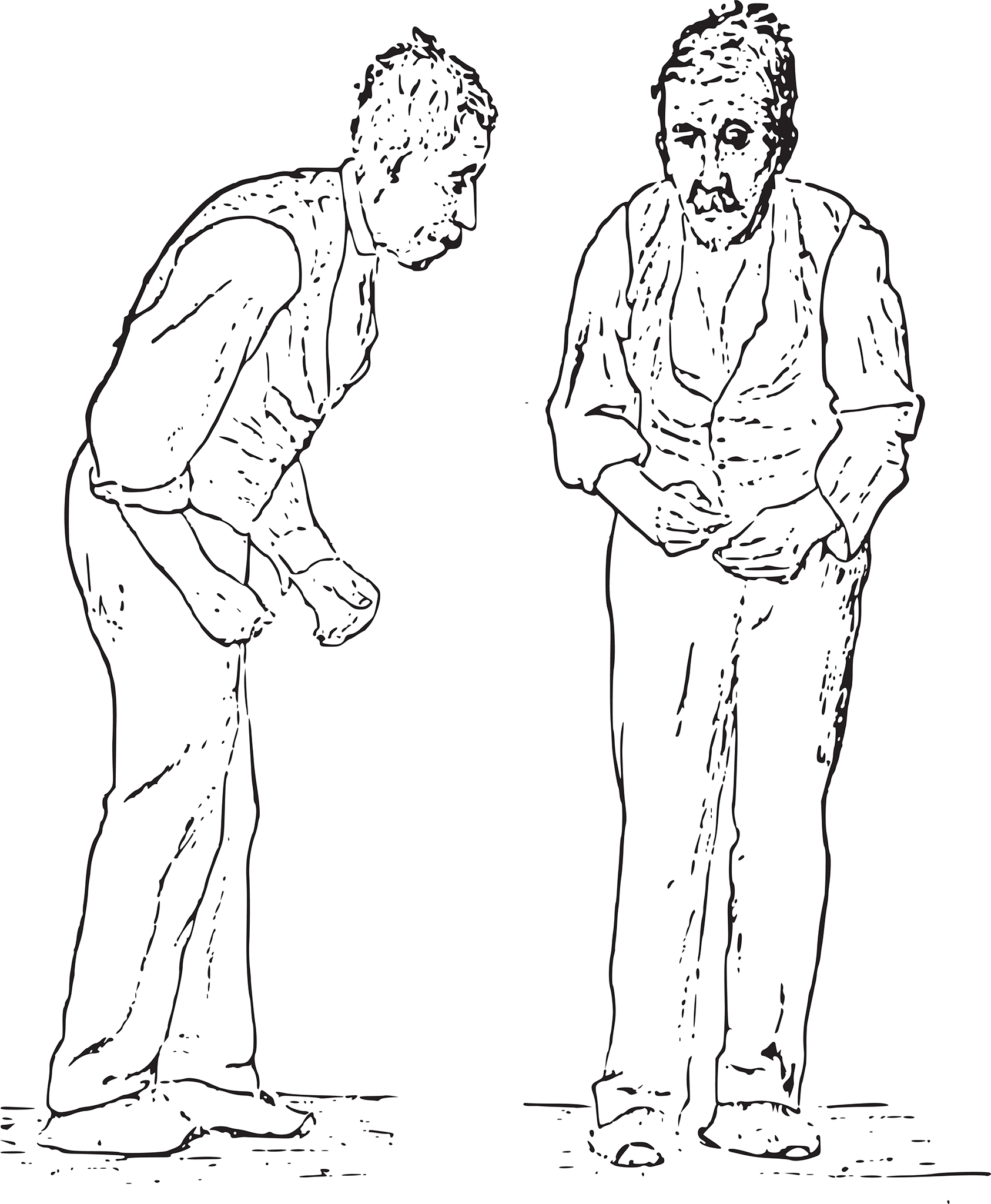
Figure 7.5. Findings of Parkinson’s Disease Note the masklike facies, shuffling gait, and stooped posture.
The biological basis of this disease is decreased dopamine production in the substantia nigra, a layer of cells in the brain that functions to produce dopamine to permit proper functioning of the basal ganglia, as shown in Figure 7.6. The basal ganglia are critical for initiating and terminating movements, as well as sustaining repetitive motor tasks and smoothening motions; thus, the symptoms of Parkinson’s disease flow logically from its underlying cause. This condition can be partially managed, therefore, with L-DOPA, a precursor that is converted to dopamine once in the brain, replacing that which is lost due to Parkinson’s disease. There have also been attempts to regenerate dopaminergic neurons in the substantia nigra using stem cells placed into the central nervous system. Similar stem cell-based therapies have been used in other contexts, such as after a spinal cord injury or stroke to attempt to regenerate function in the central nervous system, with limited results.
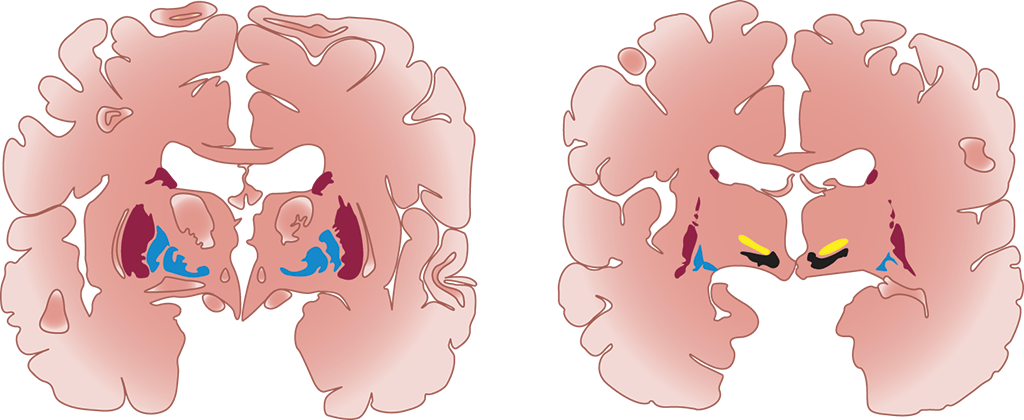
Figure 7.6. The Basal Ganglia The substantia nigra in the midbrain (black) releases dopamine to activate the other regions of the basal ganglia (blue, red, and yellow).
REAL WORLD
Note the connection between schizophrenia and psychosis (caused by an excess of dopamine) and Parkinson’s disease (caused by a deficit of dopamine). Antipsychotic medications often lead to “parkinsonian” side effects, like muscle rigidity and flattened affect. Medications used in Parkinson’s disease often lead to psychotic side effects, such as hallucinations and delusions.
MCAT CONCEPT CHECK 7.3
Before you move on, assess your understanding of the material with these questions.
- Which hormone and neurotransmitter concentrations are elevated in depression? Which ones are reduced?
____________________________
- Elevated:
_________________________
- Reduced:
- Provide an example of a genetic factor that appears to increase risk of Alzheimer’s disease. ____________________________
____________________________
- How are dopamine levels related in schizophrenia and Parkinson’s disease?
Conclusion
The content covered in this chapter will allow you to score more points on the MCAT—and to prepare for your clinical clerkships in psychiatry. This chapter is unique in that it covers not how the mind normally works, as we see in the other chapters in this book, but rather how the mind works when it is functioning abnormally. The MCAT tests critical thinking; one common way to do this is to ask what happens when a system—like the mind—is not functioning normally. Thus, this chapter covered high-yield information that is likely to appear on the MCAT because it connects all three subjects of the Psychological, Social, and Biological Foundations of Behavior section. In the next chapter, we move away from the individual as we begin to explore social psychology; from there, we’ll continue expanding outward as we move into sociology.
GO ONLINE!
You’ve reviewed the content, now test your knowledge and critical thinking skills by completing a test-like passage set in your online resources!
CONCEPT SUMMARY
Understanding Psychological Disorders
- The biomedical approach to psychological disorders takes into account only the physical and medical causes of a psychological disorder. Thus, treatments in this approach are of a biomedical nature.
- The biopsychosocial approach considers the relative contributions of biological, psychological, and social components to an individual’s disorder. Treatments also fall into these three areas.
- The Diagnostic and Statistical Manual of Mental Disorders is used to diagnose psychological disorders. Its current version is DSM-5 (published May 2013). It categorizes mental disorders based on symptom patterns.
- Psychological disorders, especially anxiety, depressive, and substance use disorders, are very common in the population.
- Psychological disorders can be treated with psychopharmacology (medication) and/or psychotherapy, which includes talk therapy techniques like psychoanalysis and behavioral therapy techniques that directly modify behavior like systematic desensitization for treating phobias. Cognitive behavioral therapy (CBT) is one popular psychotherapy that uses a hybrid approach.
Types of Psychological Disorders
- Schizophrenia is the prototypical disorder with psychosis as a feature. It contains positive and negative symptoms.
- Positive symptoms add something to behavior, cognition, or affect and include delusions, hallucinations, disorganized speech, and disorganized behavior.
- Negative symptoms are the loss of something from behavior, cognition, or affect and include disturbance of affect and avolition.
- Depressive disorders include major depressive disorder, dysthymia, and seasonal affective disorder.
- Major depressive disorder contains at least one major depressive episode.
- Persistent depressive disorder (dysthymia) is the presence of depressive symptoms for at least two years that do not meet criteria for major depressive disorder.
- Bipolar and related disorders have manic or hypomanic episodes.
- Bipolar I disorder contains at least one manic episode.
- Bipolar II disorder contains at least one major depressive episode and least one hypomanic episode.
- Cyclothymic disorder describes periods of manic and depressive symptoms that are not severe enough to be labeled an episode. These symptoms must persist for at least 2 years and be present the majority of that time.
- Anxiety disorders capture conditions in which excessive fear or anxiety impairs one’s daily functions. Anxiety disorders are differentiated by the stimuli that induces anxiety.
- Specific phobias are irrational fears of specific objects or situations.
- Separation anxiety disorder is anxiety due to separation from one’s caregivers, often with the ideation that if separated, either the caregiver or the patient will be harmed.
- Social anxiety disorder is anxiety due to social or performance situations with the ideation that the patient will be negatively evaluated.
- Selective mutism disorder is the impairment of speech in situations where speaking is expected.
- Panic disorder is marked by recurrent panic attacks: intense, overwhelming fear and sympathetic nervous system activity with no clear stimulus. It may lead to agoraphobia.
- Agoraphobia is a fear of places or situations where it is hard for an individual to escape.
- Generalized anxiety disorder is a disproportionate and persistent worry about many different things for at least six months.
- Obsessive–compulsive disorder and related disorders are characterized by perceived needs (obsessions or preoccupations) and paired actions to meet those needs (compulsions).
- Obsessive–compulsive disorder is characterized by obsessions (persistent, intrusive thoughts and impulses) and compulsions (repetitive tasks that relieve tension but cause significant impairment in a person’s life).
- Body dysmorphic disorder is characterized by an unrealistic negative evaluation of one’s appearance or a specific body part. The individual often takes extreme measures to correct the perceived imperfection.
- Hoarding disorder is characterized by the reluctance of giving up one’s physical possessions. Often this behavior is associated with excessive acquisition of physical items.
- Posttraumatic stress disorder (PTSD) is characterized by intrusion symptoms (reliving the event, flashbacks, nightmares), avoidance symptoms (avoidance of people, places, objects associated with trauma), negative cognitive symptoms (amnesia, negative mood and emotions), and arousal symptoms (increased startle response, irritability, anxiety). These symptoms can be explained from the behaviorist perspective.
- Dissociative disorders include dissociative amnesia, dissociative identity disorder, and depersonalization/derealization disorder.
- Dissociative amnesia is an inability to recall past experience without an underlying neurological disorder. In severe forms, it may involve dissociative fugue, a sudden change in location that may involve the assumption of a new identity.
- Dissociative identity disorder is the occurrence of two or more personalities that take control of a person’s behavior.
- Depersonalization/derealization disorder involves feelings of detachment from the mind and body or from the environment.
- Somatic symptom and related disorders involve significant bodily symptoms.
- Somatic symptom disorder involves at least one somatic symptom, which may or may not be linked to an underlying medical condition, that causes disproportionate concern.
- Illness anxiety disorder is a preoccupation with thoughts about having, or coming down with, a serious medical condition.
- Conversion disorder involves unexplained symptoms affecting motor or sensory function and is associated with prior trauma.
- Personality disorders (PD) are patterns of inflexible, maladaptive behavior that cause distress or impaired functioning in at least two of the following: cognition, emotions, interpersonal functioning, or impulse control. They occur in three clusters: A (odd, eccentric), B (dramatic, emotional, erratic), and C (anxious, fearful).
- Cluster A includes paranoid, schizotypal, and schizoid PDs. Cluster B includes antisocial, borderline, histrionic, and narcissistic PDs. Cluster C includes avoidant, dependent, and obsessive–compulsive PDs.
- Paranoid PD involves a pervasive distrust and suspicion of others.
- Schizotypal PD involves ideas of reference, magical thinking, and eccentricity.
- Schizoid PD involves detachment from social relationships and limited emotion.
- Antisocial PD involves a disregard for the rights of others.
- Borderline PD involves instability in relationships, mood, and self-image. Splitting is characteristic, as are recurrent suicide attempts.
- Histrionic PD involves constant attention-seeking behavior.
- Narcissistic PD involves a grandiose sense of self-importance and need for admiration.
- Avoidant PD involves extreme shyness and fear of rejection.
- Dependent PD involves a continuous need for reassurance.
- Obsessive–compulsive PD involves perfectionism, inflexibility, and preoccupation with rules.
Biological Basis of Nervous System Disorders
- Schizophrenia may be associated with genetic factors, birth trauma, adolescent marijuana use, and family history. There are high levels of dopaminergic transmission.
- Depression is accompanied by high levels of glucocorticoids and low levels of norepinephrine, serotonin, and dopamine.
- Bipolar disorders are accompanied by high levels of norepinephrine and serotonin. They are also highly heritable.
- Alzheimer’s disease is associated with genetic factors, brain atrophy, decreases in acetylcholine, senile plaques of ***β*-amyloid, andneurofibrillary tangles** of hyperphosphorylated tau protein.
- Parkinson’s disease is associated with bradykinesia, resting tremor, pill-rolling tremor, masklike facies, cogwheel rigidity, and a shuffling gait. There is decreased production of dopamine by cells in the substantia nigra.
ANSWERS TO CONCEPT CHECKS
**7.1**
- Whereas the biomedical model considers only the physical, pathological mechanisms that underlie mental illness, the biopsychosocial model considers the contributions of these biological factors along with psychology (thoughts, emotions, or behaviors) and social situation (environment, social class, discrimination, or stigmatization).
- The following disorders occur in greater than 2 percent of the United States population per year: specific phobia, social anxiety disorder, major depressive disorder, posttraumatic stress disorder, bipolar disorder, generalized anxiety disorder, and panic disorder.
**7.2**
- Positive symptoms of schizophrenia, including delusions, hallucinations (usually auditory), disorganized thought, and disorganized behavior, are likely to improve from treatment with an antipsychotic medication. Negative symptoms, including disturbance of affect and avolition, are largely unaffected by antipsychotic medications.
- Major depressive episodes include a two-week duration of at least five of the following symptoms: depressed mood, loss of interest (anhedonia), sleep disturbance, feelings of guilt, lack of energy, difficulty concentrating, changes in appetite, psychomotor symptoms, and suicidal thoughts. At least one of the symptoms must be depressed mood or anhedonia. Manic episodes include a one-week duration of at least three of the following symptoms: elevated or expansive mood, distractibility, decreased need for sleep, grandiosity, flight of ideas or racing thoughts, agitation, pressured speech, and engagement in risky behavior.
- Major depressive disorder contains at least one major depressive episode with no manic episodes. Bipolar I disorder has at least one manic episode with or without depressive episodes. Bipolar II disorder has at least one hypomanic episode with at least one major depressive episode. Cyclothymic disorder has hypomanic episodes and dysthymia that is not severe enough to be a major depressive episode.
- Obsessions are persistent, intrusive thoughts and impulses that produce tension. In this case, the obsession is the patient’s thought that someone will break into the apartment. Compulsions are repetitive tasks that relieve tension but cause significant impairment in a person’s life. This patient’s compulsion is having to check the latch on the apartment door five times before going to bed. Their relationship is that obsessions raise tension while compulsions relieve that tension.
-
Cluster Features Personality Disorders A Odd or eccentric Paranoid, schizotypal, schizoid
B Dramatic, emotional, or erratic Antisocial, borderline, histrionic, narcissistic
C Anxious or fearful Avoidant, dependent, obsessive–compulsive
**7.3**
- In depression, levels of cortisol are increased. Many neurotransmitter levels are reduced, including norepinephrine, serotonin, and dopamine.
- Mutations in the presenilin genes (chromosomes 1 and 14) and β-amyloid precursor protein gene (chromosome 21) are associated with increased risk for Alzheimer’s disease.
- Dopamine levels are elevated in schizophrenia and reduced in Parkinson’s disease. Thus, treatments for one disorder may cause symptoms similar to those of the other.
SCIENCE MASTERY ASSESSMENT EXPLANATIONS
1. C
Negative symptoms are the absence of normal or desired behavior, which include disturbance of affect and avolition. Positive symptoms are the addition of abnormal behavior, including hallucinations, (A), disorganized behavior, (B), and delusions, (D).
2. A
Echolalia is an involuntary repetition of others’ words and utterances and may be seen in schizophrenia. Echopraxia, (B), is imitation of others’ actions. Loosening of associations, (C), is a type of disordered thought in which the patient moves between remotely related ideas. Neologisms, (D), are newly invented words.
3. A
Focusing on details, loving routine, having a sense that there is only one right way to do things, and lack of humor suggests an obsessive–compulsive personality disorder.
4. C
Depression is marked by a period of at least two weeks in which the patient has five of nine cardinal symptoms, one of which must be depressed mood or lack of interest (anhedonia). While decreased need for sleep is commonly seen in manic episodes, it may also appear in depression, as sleep disturbance is one of the nine cardinal symptoms. Not all depressed individuals are suicidal, as in (B). In older individuals, depression may often manifest as anhedonia without feelings of sadness, invalidating (D).
5. B
The doctor is using the biomedical approach since the focus is on only the biological cause of the patient’s symptoms. Furthermore, since the treatment centers only on the patient, the doctor is using direct therapy. This combination of approach and therapy matches (B) as the correct answer. By contrast, a doctor using the biopsychosocial approach would likely consider the patient’s recent move, stresses associated with the accelerated program, and lack of support structure as potential causes of depression. Additionally, treatment using the biopsychosocial approach includes indirect therapy which focuses on increasing social support.
6. D
Dissociative fugue is characterized by sudden travel or change in normal day-to-day activities and occurs in some cases of dissociative amnesia. Symptoms include an inability to recall one’s past or confusion about one’s identity. Thus, the described patient is most likely to be suffering dissociative amnesia accompanied by dissociative fugue.
7. D
Agoraphobia, or a fear of places or situations in which it would be difficult to escape, is commonly seen in panic disorder. Concern about having a panic attack in public may make these individuals fearful of leaving their home.
8. D
Phobias affect approximately 9% of the population, meaning that on average 9 in 100 individuals will have some sort of phobia. In a sample of 50 people, 4 or 5 people will need to be excluded, assuming that the sample is representative of the larger population. Thus, (D) is correct.
9. A
The symptoms listed indicate a major depressive episode. However, depressive episodes can be a part of bipolar disorders, which also contain manic episodes. Thus, if manic episodes have not yet been asked about, one cannot distinguish between depression or bipolar disorder as the correct diagnosis yet.
10. B
To determine if this patient has major depressive disorder or a bipolar disorder, the presence of manic (or hypomanic) episodes should be confirmed. Bipolar disorders contain manic (or hypomanic) episodes, while major depressive disorder does not.
11. B
The correct answer should be a statement that is not relevant to Alzheimer’s disease. Choice (B), a decreased abundance of serotonin and norepinephrine, describes the monoamine theory of depression. These neurochemical changes are not known risk factors or diagnostic criteria for Alzheimer’s disease, making (B) the correct answer. The remaining choices are either risk factors or diagnostic criteria for Alzheimer’s disease. Choice (A) describes the increased risk of Alzheimer’s disease in individuals with Down syndrome, as the gene for β-amyloid precursor is on chromosome 21. Choices (C) and (D) both describe biological markers of Alzheimer’s disease.
12. B
Splitting, the consideration of others as either “all good” or “all bad,” is characteristic of borderline personality disorder.
13. A
Conversion disorder is marked by a motor or sensory symptom in the absence of an underlying physical or neurological cause. It is associated with an inciting event that, in this case, may have been the argument with the family member. The patient’s lack of concern over the deficit is referred to as la belle indifférence.
14. C
The symptoms indicate that the patient likely has Parkinson’s disease. This disease is caused by decreased dopamine production in the substantia nigra.
15. B
Bipolar disorders have been shown to be highly heritable and are associated with increased levels of norepinephrine and serotonin in the brain. Bipolar I disorder can be diagnosed with a single manic episode and does not require a major depressive episode. Bipolar II disorder requires at least one hypomanic episode and one major depressive episode. Cyclothymic disorder contains at least one hypomanic episode and dysthymia.
GO ONLINE
Consult your online resources for additional practice.
SHARED CONCEPTS
Behavioral Sciences Chapter 1
Biology and Behavior
Behavioral Sciences Chapter 3
Learning and Memory
Behavioral Sciences Chapter 12
Social Stratification
Biology Chapter 4
The Nervous System
Biology Chapter 5
The Endocrine System
Biology Chapter 12
Genetics and Evolution