Chapter 11: Social Structure and Demographics
Chapter 11: Social Structure and Demographics
SCIENCE MASTERY ASSESSMENT
Every pre-med knows this feeling: there is so much content I have to know for the MCAT! How do I know what to do first or what’s important?
While the high-yield badges throughout this book will help you identify the most important topics, this Science Mastery Assessment is another tool in your MCAT prep arsenal. This quiz (which can also be taken in your online resources) and the guidance below will help ensure that you are spending the appropriate amount of time on this chapter based on your personal strengths and weaknesses. Don’t worry though—skipping something now does not mean you’ll never study it. Later on in your prep, as you complete full-length tests, you’ll uncover specific pieces of content that you need to review and can come back to these chapters as appropriate.
How to Use This Assessment
If you answer 0–7 questions correctly:
Spend about 1 hour to read this chapter in full and take limited notes throughout. Follow up by reviewing all quiz questions to ensure that you now understand how to solve each one.
If you answer 8–11 questions correctly:
Spend 20–40 minutes reviewing the quiz questions. Beginning with the questions you missed, read and take notes on the corresponding subchapters. For questions you answered correctly, ensure your thinking matches that of the explanation and you understand why each choice was correct or incorrect.
If you answer 12–15 questions correctly:
Spend less than 20 minutes reviewing all questions from the quiz. If you missed any, then include a quick read-through of the corresponding subchapters, or even just the relevant content within a subchapter, as part of your question review. For questions you answered correctly, ensure your thinking matches that of the explanation and review the Concept Summary at the end of the chapter.
- Which of the following best describes a manifest function?
- An intended positive effect on a system
- An intended negative effect on a system
- An unintended positive effect on a system
- An unintended negative effect on a system
- Studying why a nod means “yes” in many cultures is most representative of which of the following sociological concepts?
- Demographic transition
- Expectancy theory
- Symbolic interactionism
- Demographic shift
- Which of the following ethical principles states that physicians should avoid using treatments with greater potential for harm than benefit?
- Autonomy
- Beneficence
- Justice
- Nonmaleficence
- A Cuban-American man living in the United States has the dominant physical features of a Black man. He speaks Spanish, prefers Latin foods, and listens to Latin music. His preferences are best defined through which of the following attributes?
- Race
- Ethnicity
- Culture
- I only
- II only
- II and III only
- I, II, and III
- A patient who resides in the United States says, “I love you,” and hugs the doctor after every routine visit. This behavior violates:
- personal beliefs.
- patient autonomy.
- social values.
- social norms.
- Which of the following demographics can be measured in events per 1000 people per year?
- Birth rate
- Fertility rate
- Mortality rate
- I only
- I and III only
- II and III only
- I, II, and III
- Because there are more than 500 American Indian tribes, there are several different healing practices among them. Some tribes may have ceremonies that include chanting, singing, body painting, dancing, and even use of mind-altering substances to persuade the spirits to heal the sick person. These ceremonies are examples of:
- latent functions.
- rituals.
- cultural barriers.
- social movements.
- Over the last few decades, the United States population has become:
- bigger, older, and more diverse.
- bigger, younger, and more diverse.
- smaller, older, and less diverse.
- smaller, older, and more diverse.
- Which of the following is NOT an example of material culture?
- Traditional Kenyan clothing
- Japanese cuisine
- American values
- American Indian sand paintings
- During which stage of demographic transition are both birth rates and mortality rates low?
- Stage 1
- Stage 2
- Stage 3
- Stage 4
- Shortly after a state legalizes gambling in casinos, a formal coalition forms to oppose the building of any casinos in the major cities of the state. This scenario includes:
- conflict theory.
- social institutions.
- a social movement.
- I only
- I and III only
- II and III only
- I, II, and III
- A young adult male claims to have had sexual relationships mostly with other men, although he has been attracted to women at times. What would be his most likely score on the Kinsey scale?
- 0
- 1
- 5
- 6
- Which of the following demographic variables is known to be biologically determined?
- Gender
- Sex
- Ethnicity
- Sexual orientation
- Which of the following would contribute to increasing population growth over time?
- A fertility rate less than 2
- An immigration rate larger than emigration rate
- An increase in mortality rate
- A decrease in birth rate
- Urbanization can cause all of the following negative effects EXCEPT:
- decreased opportunity for social interaction.
- increased transmission of infectious disease.
- decreased air quality and sanitation.
- increased rates of violent crime.
Answer Key
- A
- C
- D
- C
- D
- B
- B
- A
- C
- D
- D
- C
- B
- B
- A
Chapter 11: Social Structure and Demographics
CHAPTER 11
SOCIAL STRUCTURE AND DEMOGRAPHICS
In This Chapter
11.1 Sociology: Theories and Institutions
Theoretical Approaches
Social Institutions
11.2 Culture
Material and Symbolic Culture
Language
Values, Beliefs, Norms, and Rituals
Evolution and Human Culture
11.3 Demographics
Common Demographic Categories
Demographic Shifts and Social Change
Concept Summary
CHAPTER PROFILE
The content in this chapter should be relevant to about 13% of all questions about the behavioral sciences on the MCAT.
This chapter covers material from the following AAMC content categories:
7B: Social processes that influence human behavior
9A: Understanding social structure
9B: Demographic characteristics and processes
Introduction
A frail, older man is admitted to the Intensive Care Unit at a local hospital. He is gaunt, weighing just over 100 pounds, in severe respiratory distress, and nearing circulatory collapse. The intensive care team works to stabilize the patient by starting intravenous lines and pumping fluids. The patient screams statements in a language the team doesn’t speak and is eventually sedated so they can intubate and ventilate him. They begin to run tests and discover that the man has widespread metastatic lung cancer that is unlikely to be cured or even controlled through chemotherapy or radiation. The patient’s wife and children visit the next morning and are told of the bad news. After crying for some time, they turn to the intensive care team and ask them not to inform the patient of this grave diagnosis. They explain that in their culture family members are expected to make healthcare decisions for the ill to avoid burdening them with such matters. The members of the medical team, however, feel that they must adhere to the tenets of local medical ethics—and their country’s laws—and allow the patient to make his own healthcare decisions. As the head of the hospital ethics committee, you get a call from the team to help them make this decision. What would you do?
Ethicists and sociologists alike wrestle with medical dilemmas like these. As a clinician in an ever-diversifying society, you will certainly run into challenging situations like these, where you must try to balance a patient’s cultural beliefs with the processes and protocols of the healthcare system in which you work. In this chapter, we’ll explore some of the sociological topics on the MCAT, focusing on theoretical models and the key institutions on which you are likely to be tested. We’ll then explore culture itself. Finally, we’ll describe demographics, the mathematical and statistical modeling of sociological concepts.
11.1 Sociology: Theories and Institutions
LEARNING OBJECTIVES
After Chapter 11.1, you will be able to:
- Recall the primary theses of major sociological theories, including functionalism, conflict theory, symbolic interactionism, social constructionism, rational choice theory, and feminist theory
- Contrast manifest and latent functions of given elements of a sociological system
- List the four key tenets of American medical ethics
Sociology is the study of society: how we create society, how we interact within and change society, and how we define what is normal and abnormal in society. Whereas psychologists focus on the behaviors of individuals, sociologists focus on the way groups organize and interact. Of course, it would be difficult to describe society as a whole since human society is not completely uniform and is instead made up of distinct cultures, subcultures, groups, and institutions, each with its own structure, patterns, and interests. As a result, sociologists study the subject at different levels: The micro level consists of family groups and local communities. The meso level consists of organizations, institutions, and ethnic subcultures. And the macro level consists of national and international systems.
Theoretical Approaches
Because human interaction is so complex, sociologists have proposed many models, called theoretical approaches to sociology, to help analyze and explain aspects of human social behavior. Sociologists don’t necessarily disagree about which model is "best." Rather, each model was created to explain certain aspects of sociology, and is inadequate for explaining other aspects. For example, one theoretical approach we will examine is symbolic interactionism, which studies how humans interact and communicate using language, writing, and other symbols. By contrast, another approach, called conflict theory, examines how groups with little power in society can rise up and create more equality. These two models are not necessarily competing explanations. Rather, they examine such vastly different aspects of human interaction that both models are necessary!
As you read this section, keep track of which aspects of human behavior each model explains, and what the weaknesses of each model are. For example, approaches such as symbolic interactionism, social constructionism, and rational choice (exchange) theory tend to focus on society at the micro- and meso-levels. On the other hand, conflict theory, structural-functionalism, and feminist theory are more applicable at the macro-level.
Symbolic Interactionism
Communication among humans stretches far beyond just language, spoken, signed, or written. Our bodies are tools of communication through our posture, facial expressions, and informal hand gestures. We recognize and put meaning into images like the smiley face, traffic signs, or corporate logos. Sacred emblems like the cross, the Star of David, or the star and crescent communicate deep religious significance. Even our clothing can communicate meaning. Any object, image, sound, or action that carries meaning to humans is a symbol. Importantly, according to this definition, while many physical objects are symbols, a symbol need not be a physical object. For example, spoken words are symbols, and so are meaningful grunts. Body language and hand gestures are symbols. Anything that carries meaning beyond its own existence is a symbol.
Symbolic interactionism is an approach to sociology pioneered by influential sociologist George Herbert Mead that attempts to understand human action and interaction by studying the symbols we use to communicate. This theoretical approach makes three main assumptions about human behavior:
- Humans act toward symbols based on the meanings that these symbols carry.
- The meanings symbols carry come from social interaction.
- Humans interpret the meaning of symbols, and this interpretation influences action.
Therefore, according to symbolic interactionism, humans are different from lower animals in that lower animals simply respond to stimuli, while humans have the capability to interpret the stimulus first, then react. For example, a dog might bare its teeth, which is a gesture that other dogs always interpret as a symbol of aggression. Lower animals are not able to conceive of alternative meanings to gestures. By contrast, the thumbs up gesture in American culture generally signifies approval. In a different context, however, it could be used sarcastically to communicate disapproval. And in some Middle Eastern countries, it is an offensive gesture. The meaning of the thumbs up symbol therefore depends not only on social and cultural understanding, but also on a person’s interpretation.

Figure 11.1. Symbolic Interactionism Hand gestures do not always carry the same meaning across cultures. The thumbs-up is a sign of approval in American culture; in some Middle Eastern countries, it is an offensive gesture.
Not only do hand gestures carry different meanings in different cultures, but different cultures have unique languages and slang, alphabets and number systems, traffic signs, and so on. In fact, the meaning of a symbol might differ even from group to group within a culture. The shared understanding of symbols is therefore a micro- or meso-level phenomenon. One major limitation to the symbolic interactionist approach is that it overlooks macro-level structures, like cultural norms or class interactions.
Social Constructionism
The agreed-upon meaning of symbols can change. For example, the peace sign, which today is a symbol signifying peace and freedom in general, originally was used to indicate support for nuclear disarmament specifically. Society’s interpretation of the peace sign has therefore broadened over time. This example shows that the meaning of a symbol does not come from the symbol itself, but from implicit social agreement. Symbols are therefore examples of social constructs. A social construct is any idea that has been created and accepted by the people in a society. Social constructionism is the attempt to understand a society through the study of the society’s social constructs.
KEY CONCEPT
Symbolic interactionism reflects on how we use symbols to interact with each other. Social constructionism reflects on how we, as a society, construct concepts and principles.
Symbols are not the only type of social construct. Abstract ideas might also be social constructs. For example, the definitions of concepts like honor and justice rely on group agreement among individuals within a given society, and these concepts are therefore social constructs. Sociologists also apply social constructionism to physical objects, such as money. Paper money and coinage do not inherently have significant value; it is only because we, as a society, imbue these objects with value that they can be used to trade for goods and services. Other examples of social constructs include work ethic, acceptable dress, and gender roles.
As with symbolic interactionism, social constructionism is useful for explaining micro- and meso-level sociological phenomena. Any social construct depends on the society being studied, and different societies will have different social constructs. Therefore, like symbolic interactionism, a limitation of social constructionism is that this theory cannot account for macro-level sociological phenomena.
Rational Choice (Exchange) Theory
Rational choice theory is one more micro- to meso-level approach to sociology. This theory focuses on individual decision making. According to rational choice theorists, humans will make rational choices to further their own self-interests. This theory claims that people weigh the costs and benefits when making choices, ranking their options based on maximizing perceived benefit. For example, when deciding to purchase a new laptop, rational choice theory claims that a person will gather information about characteristics such as cost, performance, brand recognition, and so on, and then will rank their options and choose the best one.
This laptop example illustrates that rational choice theory is influenced by the study of economics. Rational choice theory becomes a model of sociology when this idea of rational transactions is applied to the social interaction. The rational choice perspective views all social interactions as transactions that take into consideration the benefits and harms to the individual. Every outcome in a given social interaction can be associated with particular social rewards (such as accolades, honor, prestige, or social approval) and with particular punishments (such as embarrassment, humiliation, sanctions, or stigmatization). From the rational choice perspective, an individual carefully considers all of the possible rewards and punishments of each social action and chooses the option that results in the greatest social benefit.
Moreover, according to rational choice theorists, people evaluate whether there is reciprocity and balance in social relationships: People stay in relationships because they get something from the exchange, and they leave relationships when there are more social costs than benefits. Due to this view of relationships as exchanges of social value, rational choice theory is sometimes called social exchange theory, or just exchange theory for short.
Rational choice (exchange) theory is acceptable for explaining some micro- and meso-level sociological phenomena. However, rational choice (exchange) theory does not easily explain charitable, illogical, unselfish, or altruistic behavior.
Conflict Theory
Conflict theory is a macro theory that attempts to understand society by examining the inevitable conflicts between groups in society. Conflict theory has its origins in the writings of Karl Marx, a 19th century social philosopher who examined the influence of capitalism on 19th century society. Capitalism is an economic system in which individuals and corporations, rather than governments, own and control what Marx called the means of production, meaning property, machinery, factories, or any other means of creating a saleable good or service. According to Marx, such private ownership naturally leads to a small, wealthy capitalist (bourgeoisie) class, who control the means of production. In Marx’s model, the rest of society is relegated to a lower worker (proletariat) class that performs manual labor. Because the capitalist class owns the means of production, this class has power over the worker class, and the disparity in power and resources between these two groups leads to conflict. According to Marx, the conflict in such a society would be a physical one: Eventually, the worker class would rise up and overthrow the capitalist class and form a new, classless society.
REAL WORLD
Conflict theory can be applied to healthcare and medicine. Conflict theorists would not deny that modern healthcare can help people maintain or restore their health; however, they may ask who holds the power in the healthcare system. Is it the patient? The doctor? Hospitals? Pharmaceutical companies? Insurance companies? The government? This is an issue the United States continues to grapple with.
Where Marx focused specifically on conflict between capitalists and workers, modern conflict theory expands this idea to examine any conflict between groups with more power and those with less. For example, conflict might exist between people of different generations, different religions, or different regions of a country. According to conflict theory, in any such conflict, individuals in the group with more power attempt to preserve their power by shaping the structure of society itself. The group with more power uses their influence to dictate the laws, customs, and cultural norms of the society. However, according to conflict theorists, if people in lower-status positions recognize this power differential and see that others share a common dissatisfaction, then these individuals can organize to form interest groups, through which they can use tools such as protesting or voting to enact change and equalize power. In short, according to conflict theory, for the more powerful in society, maintenance of the status quo is usually desirable, and for the less powerful, change comes through disruption and revolution.
While conflict theory is a useful model for describing many large-scale changes and other macro-level societal phenomena, it is not very effective for explaining the choices of individuals in society. Also, conflict theorists tend to focus on social stress and disharmony, so conflict theory is less effective than some other models at explaining social cohesion, cooperation, and altruism.
Structural-Functionalism
In some ways, structural-functionalism is the inverse of conflict theory. The founder of structural-functionalism, Émile Durkheim, was interested in how large societies survive over long time periods, and was therefore concerned with social cohesion and stability. Durkheim compared society to an organism and proposed that each group in society has a role to play in the overall health and operation of society. These roles might be very different, in the same way that different organs or even different cells have very different functions within an organism, but each is important. Durkheim called each social group’s role its function: the contribution made by that group to the system. According to structural-functionalist theory, the different groups of society work together in an unconscious, almost automatic way toward maintenance of equilibrium.
In structural-functionalism, functions can either be manifest or latent. A manifest function is an intended consequence of the actions of a group within a society. When an organization or institution has unintended but beneficial consequences, these are called latent functions. For example, annual meetings of medical societies have the manifest function of educating a group of physicians, sharing research findings, and setting goals for the next year. Such meetings also create stronger interpersonal bonds between physicians and provide a sense of identity for the group, both of which are latent functions. On the other hand, while both manifest and latent functions provide a benefit to society, dysfunctions are negative consequences of the existence of an institution, organization, or interaction.
Because structural-functionalism focuses on social cohesion and equilibrium, this approach is not well suited for explaining social change. Additionally, while structural-functionalism attempts to explain how groups interact with other groups, it does not explain how individuals interact within a group. To understand those kinds of micro-level interactions, other models are better suited.
Feminist Theory
Feminist theory critiques the institutional power structures that disadvantage women in society. Feminist theory was originally an offshoot of conflict theory. From a conflict theory perspective, feminist theory describes society as inherently patriarchal, with men seeking to preserve their position of power over women through societal privilege and institutional discrimination. For example, some feminist theorists argue that the study of sociology itself has been historically dominated by a male perspective.
In developed countries, gender stratification and inequality typically lessens, often as a result of the activism of feminist interest groups. However, imbalances of power still exist. In the workplace, for example, the term glass ceiling refers to processes that limit the progress of women to the highest job positions because of invisible social barriers to promotion. In contrast, even in cases where men do not seek to climb the job ladder, invisible social forces sometimes push men up to higher positions, a phenomenon called the glass escalator. The glass escalator is especially prevalent for men working in traditionally female occupations.
BEHAVIORAL SCIENCES GUIDED EXAMPLE WITH EXPERT THINKING
How does conflict theory relate to the results of this study?
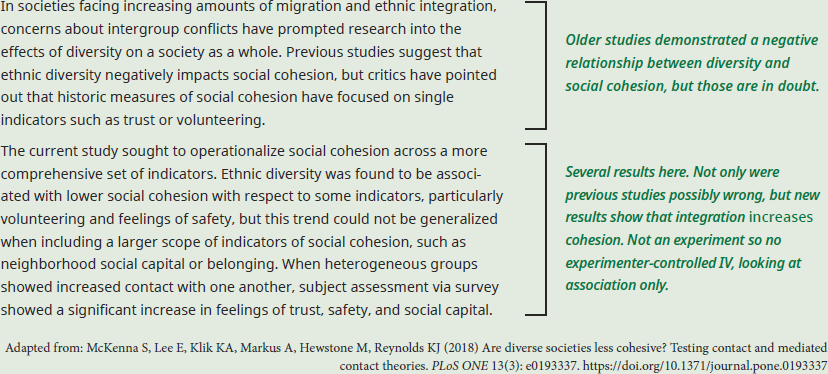
This question at first might seem tough, as the results of the study seem to suggest that there is less conflict than one would expect in more diverse societies. When faced with a question that asks us to apply a concept to a new situation, it’s useful to think critically about the definition of that concept. According to conflict theory, institutions arise as a result of power differentials between individuals, and those institutions seek to maintain that power differential.
So where is the conflict in this situation? According to the study, there can be a great deal of diversity in an area that has low interaction between different groups. In those situations, some measures of social cohesion decrease, including feelings of safety. So when people are in close quarters with diverse others, particularly when not interacting with those others regularly, perceived threat to the establishment and maintenance of the power differential will increase, which increases the conflict between groups.
However, the study also found that when people in close quarters with a diverse population interact more with diverse others, they report increased feelings of trust, safety, and social capital, indicating a reduction in perceived threat from other groups. We could infer that this increased interaction may counter the conflict theory effects noted earlier: increased trust and safety reduces fear of others, generally, and fear of loss of power, specifically. With a reduction in perceived threat and increased social cohesion, motivation for conflict should decrease, as power differentials are less threatened or groups are actively integrated into the existing power structure.
So, in summary, conflict theory provides some explanation as to why those who are not interacting with their diverse society may experience more perceived threat and conflict motivation. The study further indicates the perceived threat effect, and possibly societal conflict overall, can be countered by increased social interaction.
Social Institutions
Social institutions are well-established social structures that dictate certain patterns of behavior or relationships and are accepted as a fundamental part of culture. Social institutions regulate the behavior of individuals in core areas of society. For example, family is a social institution that encourages learning of acceptable behavior, socialization, and bonding.
Institutions exist at the meso-level of sociological analysis because they are a part of society, but are not dependent upon the individuals involved—in the United States, the idea of “government” stays basically the same even as the president, senators, representatives, and other officials change. The exact nature of each institution differs from culture to culture, although each institution performs a similar role regardless of culture. Often, institutions are dependent upon and support one another, though competition over resources can bring institutions into conflict. A summary of six of the major social institutions is provided in Table 11.1 at the end of this section.
Family
The definition of family differs greatly from culture to culture. For some, the term means “those people to whom I maintain close ties and who are related to me by blood.” For others, family is simply “the people who live in my house.” In fact, even terms for different family members (such as sister, father, cousin, and so on) are not conserved across time and culture; different patterns of kinship may be reflected by these terms. For example, it is common in Hawaiian culture to refer to all family members as cousins, while this term would not be used by many other Americans to describe one’s mother’s brother (the term uncle being preferred by many continental Americans). Different patterns of kinship between societies have bearing on responsibility for child rearing, familial loyalty, and even the boundaries of what is considered incest.
Regardless of the definition, family is the most basic of institutions. It is the institution most closely tied to the individual and helps to meet many of our most basic needs, especially when we are young, providing food, shelter, emotional and physical security, and intimacy. Additionally, many life rituals and rites of passage, such as marriage, funerals, and graduations occur in the context of family.
BRIDGE
Families help to meet many of the basic needs at the base of Maslow’s hierarchy pyramid. Maslow’s hierarchy of needs is discussed in chapter 5 of MCAT Behavioral Science Review.
Sociologists studying family relationships may examine the stages of coupling (courtship, cohabitation, engagement, and marriage), changes in relationships between spouses through time, or parenting. Parenting is a complex topic that involves socialization of children; varied definitions of the role of father, mother, and child; and single parenting, same-sex parenting, adoption, and foster parenting. Not all families are composed of a mother, a father, and children. Alternative forms exist, including single-parent families; families that cohabitate with other family members beyond the nuclear family, such as grandparents, aunts, uncles, cousins, godparents, and surrogate kin; and families with marital disunions (divorce). A number of different family structures are illustrated in Figure 11.2.

Figure 11.2. Various Family Structures
Divorce rates in the United States rose significantly in the second half of the twentieth century but have started to drop over the last two decades.
MCAT EXPERTISE
The MCAT will not expect you to know any specific demographic numbers for the exam, but you should be familiar with some of the recent trends seen in the United States population.
While the family can be a source of joy and support, it can also be a source of violence. Spousal abuse (domestic violence) is seen across all social classes and genders and can include not only physical violence, but sexual abuse, emotional abuse, and financial abuse. Domestic violence is the #1 cause of injury to American women, and is most common in families with drug abuse, especially alcoholism. Victims of domestic violence may find it challenging to leave the abusive relationship for a variety of reasons, including lack of a safe haven to escape to, financial restrictions, and psychological disorders (consider the connection to learned helplessness, described in Chapter 6 of MCAT Behavioral Sciences Review). Elder abuse is also seen across all socioeconomic classes, and most commonly manifests as neglect of an older relative—although physical, psychological, and financial abuse may occur as well. The caretaker of the individual is most commonly the source of abuse. Finally, child abuse also most commonly manifests as neglect, although physical, sexual, and psychological abuse are also common. During medical school, you will be trained to recognize certain signs suggestive of nonaccidental trauma, such as a broken femur in a child who is too young to have begun walking or burn marks on the buttocks from placing a child in scalding water. As a physician, you will be considered a mandated reporter, which means that you are legally required to report suspected cases of elder or child abuse. Domestic abuse does not fall under mandated reporting laws, but counseling and information about shelters for victims of intimate partner violence should be provided.
Education
Education, as an institution, aims to provide a population with a set of skills that will be useful to them or to society. In many societies, education is formal—in other words, it takes place in a setting designated for educational purposes using a prescribed curriculum. The function of formal education is to teach skills, facts, and mental processes, but the system also has a social latent function, providing opportunities for peer socialization and reinforcing social stratification, both within individual schools and through comparisons between schools. Education, therefore, includes not only the information and cognitive skills students learn but also the hidden curriculum of transmitting social norms, attitudes, and beliefs to students. Sociological investigations into education may focus on the ethics, morals, practices, political influence, finances, and values of an education system. Sociologists also explore educational trends, including grade inflation and deflation, adult education, online education, and accessibility of education.
Performance in the education system depends not only on a student’s intrinsic abilities, but also on the education system itself. Teacher expectancy refers to the idea that teachers tend to get what they expect from students. Thus, a teacher who places high demands on students—but who also believes that students can rise to the challenge—will more often see students succeed than a teacher who places the same demands but doubts that the students can achieve them. This is an example of a self-fulfilling prophecy, discussed in Chapter 10 of MCAT Behavioral Sciences Review, and may be due to differences in how teachers motivate, interact, and offer feedback to their students.
Education is susceptible to inequalities across socioeconomic class. Lower socioeconomic status is associated with decreased accessibility to and quality of education. This is not an easy trend to reverse. Low funding, deprioritization of education, and poor historical performance can make it challenging for a failing school district to acquire resources and improve education to its students.
As mentioned earlier, institutions are intentionally or unintentionally connected, and there is a well-known, persistent association between education and medicine. Health disparities between more educated and less educated individuals are significant, and lack of education may be a hurdle to accessing or trusting healthcare providers.
Religion
As an institution, religion is a pattern of social activities organized around a set of beliefs and practices that seek to address the meaning of existence. Religiosity refers to how religious one considers oneself to be, and includes strength of religious beliefs, engagement in religious practices, and attitudes about religion itself.
More than 80% of the global population identifies with a religion. Most follow either Christianity or Islam; other world religions include Hinduism, Buddhism, Sikhism, and Judaism. These religions are generally divided into multiple denominations or sects that may share certain beliefs and practices but not others. A denomination is simply a part of a church, a term which can refer both to a large, universal religious group and to the building in which the congregation of such a group meets. Orthodox and Reform are examples of Jewish denominations, and the Sunni and Shia are examples of Islamic denominations. Denominations often coexist, but can come into conflict when their religious beliefs promote opposing values. Whereas the word sect was historically a pejorative term, it now refers more properly to a religious group that has chosen to break off from the parent religion. The Amish would be considered a sect of Christianity. In rare cases, a religious sect may take on extreme or deviant philosophies and transform into a cult.
As the twenty-first century continues, religious groups—many of which have existed in more or less the same form for thousands of years—grapple with finding a place in contemporary society. For many religious groups, this is reflected by a shift toward modernization within the religion and relaxing historical practices. For others, there is a shift away from religion as society secularizes, or moves from a world dominated by religion toward rationality and scientific thinking. For other groups, maintenance of strict adherence to religious code, or fundamentalism, predominates.
While spirituality and religion are not equivalent terms, they are often linked to each other because they both seek to understand the meaning of existence and to identify what is sacred. Spirituality and religion may play a role in a patient’s understanding of disease, may impact healthcare decisions, and can be an essential component of the patient’s coping mechanisms.
Government and Economy
Government and economy can be defined as systematic arrangements of political and capital relationships, activities, and social structures that affect rule making, representation of the individual in society, rights and privileges, division of labor, and production of goods and services. Notably, political and economic institutions impact all other institutions to some extent. That is, the government may sanction or define specific family structures, may finance and regulate education, may recognize some religions but not others, and may play a key role in funding and certifying healthcare and medicine. The effects of the economy on institutions can also be viewed from the individual level. For example, when the economy takes a downturn, large swaths of the population may have trouble supporting their families and paying for health insurance. Note that this institutional influence is bidirectional: because of the economic downturn and changes in family, education, or health, an individual may choose to vote a new political candidate into office, or to support or oppose a particular piece of legislation.
While an in-depth exploration of the American (or any other) government is outside the scope of the MCAT, you could be asked to distinguish between different types of government. A democracy allows every citizen a political voice, usually through electing representatives to office (i.e., a representative democracy). Monarchies include a royal ruler (a king or queen), although the ruler’s powers may be significantly limited by the presence of a constitution, a parliamentary system, or some other legislative body. A dictatorship is a system where a single person holds power, and usually includes mechanisms to quell threats to this power. A theocracy is a system where power is held by religious leaders. Many of these systems of leadership are based around a charismatic authority (a leader with a compelling personality).
In comparative economics, the largest division is between capitalist and socialist economies. Capitalist economies focus on free market trade and laissez-faire policies, where success or failure in business is primarily driven by consumerism with as little intervention from central governing bodies as possible. In capitalism, a private owner or corporation maintains and profits from the success of the business. Capitalist societies encourage division of labor, where specific components of a larger task (say, developing, manufacturing, quality testing, and marketing goods) are separated and assigned to skilled and trained individuals. This promotes specialization and efficiency. Socialist economies, on the other hand, treats large industries as collective, shared businesses, and compensation is provided based on the work contribution of each individual into the system. Profit, then, is distributed equally to the workforce. There are many other forms of government and economy, but these would be defined and explained if necessary on Test Day.
Healthcare and Medicine
The institutions of healthcare and medicine are aimed at maintaining or improving the health status of the individual, family, community, and society as a whole. Healthcare is an ever-changing field, but some of the key goals in American healthcare over the past few decades include:
- Increased access to care
- Decreased costs of healthcare
- Prevention of disease before it occurs
- Association of patients with a primary care physician or a patient-centered medical home
- Increased education for the public with public health outreach
- Decreased paternalism (doctor knows best mentality)
- Reduced economic conflicts of interest for physicians
- Life course approach to health (maintaining and considering a comprehensive view of the patient’s history beyond the immediate presenting symptoms)
There has also been a shift in the role of the patient in the medical system. In the mid-twentieth century, sociologists believed that a patient who is ill takes on what was called the sick role. These sociologists believed that such patients are not responsible for their illness and are exempt from normal social roles. But on the other hand, these sociologists also believed that a patient had the obligation to want to become well and to seek out competent help. While this paradigm still exists, patients are now expected to take more ownership of their health through diet, exercise, seeking help before it is needed (through annual primary care visits and screenings), and so on. Modern sociologists also recognize that the notion that patients should feel an obligation to want to become better does not fit patients with chronic, long-term, or permanent conditions.
Even our understanding of disease has shifted over time. On the one hand, many ordinary parts of the human condition, including the full range of sexual orientations and gender identities, are no longer defined as medical conditions, as they misguidedly were in earlier editions of the DSM. On the other hand, other types of behaviors have become medicalized, meaning that they are now defined and treated as medical conditions. This latter shift can be seen in the addition of a number of diagnostic entities to the DSM-5, such as hoarding disorder and binge eating disorder.
The medical community also now recognizes that health is not only characterized by physiological wellness or disease, but also by a person’s subjective experience of their health. The phrase illness experience refers to the ways in which people, rather than doctors, define and adjust to changes in their health. For example, people can experience disease without illness, as is the case for someone living a full and productive life with a manageable condition such as HIV. People can also experience illness without disease, such as when a person experiences somatic symptoms as a result of psychological stress.
Sociologists studying healthcare are often interested in social epidemiology. Epidemiology is the study of health and its determinants within a society (discussed in detail in Chapter 12 of MCAT Behavioral Sciences Review); social epidemiology is specifically the study of the effects of institutions, social structures, and relationships on health. Social epidemiologists study the effects of racial and economic inequality or government safety net legislation on health and access to healthcare. They might also be interested in how social conditions early in life affect healthcare outcomes later.
In addition, many sociologists investigate medical ethics. In the United States, physicians are expected to adhere to four key tenets of medical ethics:
- Beneficence: the physician has a responsibility to act in the patient’s best interest.
- Nonmaleficence: do no harm; the physician has a responsibility to avoid treatments or interventions in which the potential for harm outweighs the potential for benefit.
- Respect for patient autonomy: the physician has a responsibility to respect patients’ decisions and choices about their own healthcare. While there are exceptions to this rule (significant psychiatric illness interfering with decision-making capacity, children, public health threats), patients do have the right to refuse life-saving therapies.
- Justice: the physician has a responsibility to treat similar patients with similar care, and to distribute healthcare resources fairly.
Table 11.1. Social Institutions
SOCIAL INSTITUTION NEEDS MET BY INSTITUTION STATUSES VALUES NORMS
Education Transmit knowledge and skills across generations Teacher, student, dean, principal Academic honesty, good grades Doing homework, preparing for lectures, being kind to other students
Family Regulate reproduction, socialize and protect children Father, mother, son, daughter, brother, sister, uncle, aunt, grandparent Sexual fidelity, providing for children, keeping a clean home, respect for caregivers Having as many children as one desires, being faithful to one’s spouse
Religion Concerns about life and death, the meaning of suffering and loss, desire to connect with a creator Clergy, worshipper, teacher, disciple, missionary, prophet, convert God and holy texts should be honored Going to services, following teachings of the religion, applying beliefs outside of worship
Government Maintain social order, enforce laws President, senator, lobbyist, voter, candidate Transparency, accountability, professionalism Acting in the best interest of constituents, debating political issues
Economy Organize money, goods, and services Worker, boss, buyer, seller, creditor, debtor, advertiser Making money, paying bills on time, producing efficiently Maximizing profits, the customer is always right, working hard
Medicine Heal the sick and injured, care for the dying Doctor, nurse, pharmacist, insurer, patient Hippocratic oath, staying in good health, following care providers’ recommendations Beneficence, nonmaleficence, respect for autonomy, justice
MCAT CONCEPT CHECK 11.1
Before you move on, assess your understanding of the material with these questions.
- What are manifest and latent functions?
________________________________
- Manifest functions:
_________________________
- Latent functions:
- For each of the theoretical approaches listed below, what is the primary thesis or idea of the theory?
Theoretical Approach Primary Thesis or Idea Functionalism Conflict theory Symbolic interactionism Social constructionism Rational choice-exchange theory Feminist theory
- What are the four key tenets of American medical ethics? Provide a short description of each.
Ethical Principle Description
11.2 Culture
LEARNING OBJECTIVES
After Chapter 11.2, you will be able to:
- Distinguish between material and symbolic culture
- Recall the definitions of, and the differences between, the values, beliefs, norms, and rituals of a culture
The study of culture is likely the most diverse and complex dimension within sociology. Culture can be defined as encompassing the entire lifestyle for a given group. It binds our nation-states, political institutions, marketplaces, religions, and ideologies. Culture flavors our interpretations of the world, and is generally passed through familial lines. In short, culture is what makes human societies unique from one another.
BRIDGE
A description of culture in the context of group processes is described in Chapter 8 of MCAT Behavioral Sciences Review
MCAT EXPERTISE
Ethnography is the study of cultures and customs, and ethnographic methods are experimental methods used to study the ethnicity or culture of a group.
Material and Symbolic Culture
Sociologists view culture according to two different categories: material culture and symbolic culture.
BRIDGE
Symbols are also discussed in Chapter 6 of MCAT Behavioral Sciences Review
Material Culture
One can discern a lot about people by looking at their artifacts: material items that they make, possess, and value. This examination surrounds material culture, which includes the physical items one associates with a given group, such as artwork, emblems, clothing, jewelry, foods, buildings, and tools. Sociologists explore the meaning of these objects to a given society.
An example of material culture in the United States is the American flag. This item is used to reinforce a sense of belonging via shared American citizenship. Other symbols that are considered traditionally American include barbecue, baseball, apple pie, and rock and roll.
Material culture is often most visible during ceremonies, such as birthdays, weddings, and funerals. Some artifacts of traditional Indian material culture are shown in Figure 11.3.

Figure 11.3. Material Culture Material culture includes objects important to a group, including clothing, jewelry, cuisine, ceremonial objects, and so on.
Symbolic Culture
Symbolic culture, also called nonmaterial culture, focuses on the ideas that represent a group of people. These may be encoded in mottos, songs, or catchphrases, or may simply be themes that are pervasive in the culture. Phrases like free enterprise and life, liberty, and the pursuit of happiness are examples of American symbolic culture. Material culture is often the tangible embodiment of the underlying ideas of symbolic culture.
KEY CONCEPT
Material culture is associated with artifacts (objects). Symbolic culture is associated with ideas.
For any social group to remain connected over time, there must be a culture that binds its members together. In times of war and crisis, governments often draw upon symbolic culture to rally people to action, using songs, parades, discussion of heroes past, and so on, as shown in Figure 11.4. It is not a coincidence that most high schools have a school mascot, school colors, and a school song. Such cultural artifacts are in place to help create a shared sense of identity, loyalty, and belonging. Symbolic culture includes both cognitive and behavioral components; that is, it informs cultural values and beliefs, as well as cultural norms and communication styles.

Figure 11.4. Symbolic Culture Symbolic culture includes ideas that identify a culture; it may be drawn upon to encourage loyalty or patriotism, as shown here.
Symbolic culture is usually slower to change than material culture, which can lead to the phenomenon of culture lag. The expansion of devices and technology in contemporary times are prototypical examples of culture lag: whereas American culture still prizes individuality and privacy, the development of smartphones and social media push toward a more community-oriented and less private world. Still, there is evidence that symbolic culture is beginning to change in response to these technological (material) innovations: younger generations appear to be less concerned about what personal information is publicly accessible than older generations.
Language
Language is the most highly developed and complex symbol system used by most cultures. Language consists of spoken, written, or signed symbols, which are regulated according to certain rules of grammar and syntax. Language enables us to share our ideas, thoughts, experiences, discoveries, fears, plans, and desires with others. Written language extends our capacity to communicate across both spatial and temporal boundaries. Without language, it would be difficult to transmit culture. Understanding a group’s language is critical to understanding its culture.
BRIDGE
Language is critically important in the transmission of culture. It requires a complex interplay of multiple brain circuits, which are discussed in Chapter 4 of MCAT Behavioral Sciences Review.
Values, Beliefs, Norms, and Rituals
An important component of culture are the rules that structure society. Values are what a person deems important in life, which dictates one’s ethical principles and standards of behavior. A belief is something that an individual accepts to be truth. Every culture has its own beliefs and value systems. This will be important in your future career, as patients tend to carry their beliefs into the healthcare system. For example, as described in the chapter introduction, some Asian cultures believe that healthcare decisions should be the responsibility of a patient’s family, which avoids burdening the patient (who is already ill) with having to make such a decision. This belief is in direct contrast to the American belief that patient autonomy should be prized and that healthcare decisions should be made by a patient whenever possible. These conflicts can prove challenging to healthcare professionals, and there is not always one correct answer to such dilemmas. Such situations—when a cultural difference impedes interaction with others—are called cultural barriers.
REAL WORLD
Many health systems have an ethics board to deal with conflicts that may arise from differences in belief systems between patient and practitioner, among other ethical issues. These committees tend to facilitate discussion, rather than simply issuing a decision.
As described in Chapter 8 of MCAT Behavioral Sciences Review, norms are societal rules that define the boundaries of acceptable behavior. While norms are not laws, they do govern the behavior of many individuals in society and provide a sense of social control. Norms are what provide us with a sense of what is appropriate, what we should do, and what we should not do. Norms exist for behavior, speech, dress, home life, and more.
A ritual is a formalized ceremony that usually involves specific material objects, symbolism, and additional mandates on acceptable behavior. Rituals tend to have a prescribed order of events or routine. These rituals can be associated with specific milestones, such as a baby-naming, graduation ceremony, wedding, or funeral; with holidays, such as a Thanksgiving dinner, trick-or-treating on Halloween, or a Passover seder, shown in Figure 11.5; or with regular activities, such as a Catholic mass, a pregame pep rally, or even just getting ready in the morning (showering, brushing teeth, eating breakfast, and so on).

Figure 11.5. A Passover Seder Is an Example of a Ritual Seder means “order” in Hebrew; most rituals have a specific order of events.
Evolution and Human Culture
Evolution may have selected for the development of culture. Culture serves as a method of passing down information from generation to generation; in prehistoric times, the transmission of information through culture served to teach future generations how to create tools, hunt, domesticate animals, and grow crops. Culture also creates a sense of loyalty and allegiance, which, as described in Chapter 10 of MCAT Behavioral Sciences Review, may help explain altruistic behavior. Finally, culture creates a sense of us vs. them, which presumably served a role in the dispersion of populations across the globe in different environmental niches.
Culture, in turn, may also influence evolution. There is evidence that some genetic traits may have been favored because of cultural values and beliefs. For example, human beings—at least those who are not lactose intolerant—are the only animals that are able to digest milk after adolescence; they are also the only animals that ingest another animal’s milk. These evolutionary adaptations may have arisen out of Northern European cultures, which relied heavily on cattle farming for sustenance. A mutation permitting digestion of milk into adulthood presumably imparted a nutritional and survival advantage to certain individuals, and would thus be retained within the population.
MCAT CONCEPT CHECK 11.2
Before you move on, assess your understanding of the material with these questions.
- What are material and symbolic culture?
________________________________
- Material culture:
_________________________
- Symbolic culture:
________________________________
- What is the difference between a value and a belief?
11.3 Demographics
LEARNING OBJECTIVES
After Chapter 11.3, you will be able to:
- Distinguish between race and ethnicity
- Describe symbolic ethnicity
- Describe fertility rate, birth rate, and mortality rate and how they shift during a demographic transition
- Recall examples of proactive and reactive social movements and how the two types of movements differ
Demographics refer to the statistics of populations and are the mathematical applications of sociology. Demographics can be gathered informally, such as a professor asking how many freshmen, sophomores, juniors, and seniors are in a given course, or may be gathered formally. For example, the United States Census Bureau gathers demographic data about every individual in the country every ten years.
Common Demographic Categories
Demographers can classify individuals based on hundreds of different criteria. The MCAT will not expect you to know advanced topics within demographics, but familiarity with some of the common demographic categories as well as their implications on society and healthcare are important. In this section, we’ll explore age, gender, race and ethnicity, sexual orientation, and immigration status.
Age
Aging is a inevitable process experienced by all people around the world. In this section we will explore the implications of an individual’s age on healthcare, then dive deeper into its implications on society.
Considering an individual’s age and cumulative life experiences when analyzing their personality, social status, health, and other social metrics is known as the life course perspective (sometimes referred to as the life course approach). For example, in healthcare, a psychiatrist may consider a patient’s early life events and how those events continue to impact a patient’s condition. Or perhaps a general practitioner chooses to conduct additional lung screenings on a patient who previously worked in a coal mine. In both these examples, the physician is incorporating the life course perspective into the treatment of the patient.
With the potentially large difference in the experiences between age cohorts, prejudice or discrimination based on a person’s age can arise. This is known as ageism and can be seen at all ages. For example, young professionals entering the workplace are often viewed as being inexperienced, and their opinions and ideas may therefore be ignored or downplayed. Older individuals may be perceived as frail, vulnerable, or less intelligent, and may thus be treated with less respect.
In order to understand and analyze age-related differences, researchers can group individuals based on their age or birth year; these groupings are known as age cohorts (sometimes called generational cohorts). The utility of age cohorts goes beyond understanding the differences of an individual’s life course, as they allow researchers to look at a population at a macroscopic level. An analysis of a population’s distribution among its age cohorts can predict demographic shifts, such as an aging population, the shift from a developing to developed economy, or a stable population. We’ll explore examples of each below.
REAL WORLD
The demographic tool of age cohorts has woven its way into our everyday language. If you’ve heard terms like the Silent Generation, Baby Boomers, Generation X, Millennial (Generation Y), and Generation Z, then you’ve encountered age cohorts. These generational terms group individuals by their birth year. However, age cohorts can be used to group individuals based on their current age, such as 0-14, 15-30, etc.
In the United States, many sociologists document a “graying of America” as the Baby Boomer generation ages. The term Baby Boomer stems from the large spike in fertility rates (birth rates) after World War II, or in other words, a “boom of babies.” Due to the baby boom spanning from the 1940s to 1960s, over 70 million Americans will be 65 or older by 2030, representing nearly 20 percent of the population. Thus, the fastest-growing age cohort in the United States is the 85-or-older group. This has profound effects on healthcare: more than 40 percent of adult patients in acute care hospital beds are 65 or older. Considering this shift in demographics, government programs such as Medicare and Social Security will experience increased demand, which may pose challenges for these programs.
This situation is an application of the dependency ratio, which is the ratio of the number of members of a population that are not in the workforce to the number of members that are in the workforce. This ratio depends on two components, the youth ratio and age dependency ratio. The youth ratio is defined by the number of people under the age of 15 divided by the number of people aged 15-65. The age dependency ratio is defined by the number of people over 65 divided by the number of people aged 15-65. Applied to societies, the dependency ratio quantifies the economic burden felt by the working age population (15-65) in order to support the portion of the population outside of the workforce (under 15 and over 65).
In contrast to the United States, developing countries, such as Uganda, see the reverse trend with 48% of the population being under the age of 15 years old, resulting in a dependency ratio of about 1 (2% of the population is 65 years and over, which means the dependent population roughly equals the working age population). This can be explained by the country’s steadily dropping infant mortality rate over the last several decades. Forecasting the next 10 to 20 years for Uganda would predict a large proportion of the population entering the working-age age cohort. Although this may lead to an increase in the country’s economic productivity, this demographic shift must be matched with job growth. If that does not occur, unemployment rates will increase, which could lead to civil unrest or other negative outcomes. This shift from developing to developed country is explained by demographic transition theory, covered later in this chapter.
Finally, when a population’s fertility rate and mortality rate remain relatively consistent over a long period of time, the distribution of the population among the age cohorts remains fairly constant. This is known as a stable population.
Gender
Sex and gender are not synonymous terms. Sex is a biological category. In many species, including humans, a phenotypical female is an individual that produces the larger gamete (the ovum) and carries offspring. Gender refers to a society’s notions of femininity, masculinity, and other sexual identities. Gender is therefore a socially constructed set of ideas about what it means to be male, female, or otherwise in a given culture. A culture’s ideas about gender usually include expected behavioral traits associated with a particular sex. These expected behavioral traits are known as gender roles. As such, gender roles are also social constructs. Once an individual understands these socially constructed behavioral expectations, an individual can adopt behaviors that project the gender that individual wishes to portray, which is known as the individual’s gender identity.
Gender segregation is the separation of individuals based on perceived gender. Such segregation includes divisions of male, female, and gender-neutral bathrooms, or separating male and female sports teams. Differences between genders and the phenomenon of gender segregation do not necessarily imply inequality, although inequality can occur. Gender inequality is the intentional or unintentional empowerment of one gender to the detriment of others. In the presence of gender inequality, gender stratification may occur. Gender stratification is defined as any inequality in access to social resources that is based on gender, and is an example of social stratification in general, which will be studied in Chapter 12 of MCAT Behavioral Sciences Review. To illustrate the difference between gender segregation and gender stratification: Single-gender schools are an example of gender segregation. Children enrolled in such schools do not necessarily receive unequal qualities of education. However, if there is a systemic difference in resource allocation between single-gender schools, the result is uneven access to resources, leading to gender stratification.
Race and Ethnicity
The definition of race has changed through recent history, and continues to change. The term originally referred to speakers of a common language, and later indicated national origin. However, the term has also historically been used to denote certain shared phenotypic similarities between people. The five racial categories currently recognized by the U.S. Census exemplify these shifting definitions of race. These categories are: White, Black, Asian, American Indian or Alaskan native, and Native Hawaiian / Pacific Islander. Observe that some of these racial categories, like White and Black, describe phenotypic similarities, while other categories, like American Indian and Pacific Islander, are based on national origin. Furthermore, no other country uses these same five racial labels, and in fact the officially recognized races differ in each country. So, there is no uniform agreement about racial categories; rather each society generates its own racial labels, making race a social construct. The social process by which racial groups are associated with specific attributes or characteristics is called racialization.
If race is not consistently defined, then why do sociologists concern themselves with this concept? The answer is that racial labels, though socially constructed, do materially affect the lives of people through institutionalized practices of preference and discrimination. In order to define race more scientifically, sociologists specify that the term race refers to socially constructed groupings of people based specifically on inherited phenotypic characteristics. Note that the human history of migration and mixing of populations means that there are few if any genetically isolated people left on earth. So sociologists recognize that scientifically categorizing people by genetic differences is not possible. Nevertheless, societies continue to generate racial labels based on perceived phenotypic differences, and so sociologists study how each society treats its socially defined racial groups.
An important takeaway from the above discussion is that sociologists narrow the definition of the term race to refer specifically to attempts to group people by phenotypic difference. However, sociologists recognize that societies also group people by shared language, cultural heritage, religion, and/or national origin. The term sociologists use for these types of groupings is ethnicity. While certain ethnicities are often associated with certain racial labels, race and ethnicity are distinct. Here is an illustration of the difference: African American individuals, African immigrants, and West Indian immigrants speak different languages and express different cultural norms. These three groups represent three different ethnicities. However, due to some phenotypic similarities shared by some members of these groups, individuals in these groups would generally be given the same racial label. Like race, ethnicity is also a social construct, in that ethnic labels and the criteria for inclusion in a certain ethnic group change from society to society and change over time.
REAL WORLD
Certain racial and ethnic groups have higher incidence of specific health problems. For example, the Chinese population accounts for a disproportionate number of chronic hepatitis B infections and liver cancer. Mediterranean and African populations have a significantly higher rate of hemoglobinopathies (diseases related to hemoglobin). The Ashkenazi Jewish population has a higher rate of autoimmune diseases. Some American Indian populations are associated with gallbladder and biliary tree diseases. Being of a particular race or ethnicity is not necessary for the development of any disease, but may certainly be associated with increased risk.
Symbolic ethnicity describes a specific connection to one’s ethnicity in which ethnic symbols and identity remain important, even when ethnic identity does not play a significant role in everyday life. For example, many Irish Americans in the United States celebrate their heritage only one day per year: St. Patrick’s Day. In all other facets of life, these individuals’ Irish-American ethnicity does not play a significant role. Other examples include attending folk festivals, visiting specific cultural locales for holidays, or participating in an ethnic celebration.
It is important to consider how race and ethnicity may affect one’s ability to receive proper healthcare. The Agency for Healthcare Research and Quality (AHRQ), a government agency, reports that race and ethnicity influence a patient’s chance of receiving many specific procedures and treatments. Whether due to conscious or unconscious bias, there is evidence that different races are not always offered the same level of care escalation in a medical emergency.
BRIDGE
Many public health outreach efforts are aimed at closing the gap in health disparities between populations. Health and healthcare disparities are discussed in Chapter 12 of MCAT Behavioral Sciences Review.
On the other hand, there are a number of public health outreach projects that target at-risk racial or ethnic populations through education, screening, and treatment. These specific strategies are geared to close gaps in health disparities. Many large university health systems run free clinics in local neighborhoods and may target specific populations; for example, some of these clinics will staff Spanish-speaking doctors and medical students to cater to the Hispanic immigrant population.
Sexual Orientation
Sexual orientation can be defined as the direction of one’s sexual interest. In scientific and healthcare communities, sexual orientation has historically been divided into three categories:
- Heterosexual: attraction to individuals of a different sex
- Bisexual (or pansexual): attraction to members of multiple sexes
- Homosexual: attraction to individuals of the same sex
Sexual orientation involves a person’s sexual feelings and may or may not be a significant contributor to that person’s sense of identity. It may or may not be evident in the person’s appearance or behavior. Disclosure of minority sexual orientations, sometimes called coming out of the closet, can be a major milestone in the absorption of sexuality into one’s identity. This disclosure has also been shown sometimes to have therapeutic effects: coming out is associated with decreases in depressive and anxious symptoms linked to cortisol levels and stress.
Human sexuality continues to be an important area of research for psychologists, sociologists, and biologists alike, but evidence shows that sexuality is likely more fluid than previously believed. Alfred Kinsey was a pioneer in this area, and—in addition to a number of other models and publications—described sexuality on a zero to six scale, with zero representing exclusive heterosexuality and six representing exclusive homosexuality. When ranked on this Kinsey scale, few people actually fell into the categories of zero and six, with a significant proportion of the population falling somewhere between the two.
Sexual and gender identity minorities are often grouped together under the umbrella term LGBTQ (lesbian, gay, bisexual, transgender, and queer or questioning). In some cases, this acronym has been expanded to include other self-definitions of sexuality and sexual identity, including I (intersex) or A (asexual).
Several health disparities have been recognized within the LGBTQ community. The most significant historical disparity is HIV, which disproportionately affected individuals who are gay in urban environments during the early 1980s. While the prevalence of HIV is still slightly higher in men who have sex with men (MSM), it exists in all populations. Efforts to encourage safe sex and increase screening have helped to slow the epidemic of HIV, as has increased awareness of those with HIV/AIDS with projects like the AIDS Memorial Quilt, shown in Figure 11.6. Within the healthcare system, individuals who are lesbian receive less screening for cervical cancer and may not be screened for other sexually transmitted infections. Individuals who are transgender have multiple areas of increased risk, including off-label or unsupervised use of “street hormones” without proper counseling on their side effects.

Figure 11.6. The AIDS Memorial Quilt
Mental health disparities are also common in the LGBTQ community. LGBTQ youth are at significantly higher risk for bullying, victimization, and violence, and have higher rates of suicide. In adults, the LGBTQ population has a higher prevalence of depression and anxiety than their heterosexual and cisgender counterparts. In addition, men who are gay have an increased rate of eating disorders as compared to men who are heterosexual. A host of campaigns and outreach efforts have begun to target these disparities.
Immigration Status
According to the US Census Bureau, the nation’s total recent immigrant population is growing rapidly; it was quantified at 40.4 million in 2011 and is expected to increase by roughly 20 million in the next two decades. This tells us that immigrants, whether documented or undocumented, are interwoven into every social structure and institution in the United States. The nativity of immigrant populations changes over time; in the most recent census, the largest proportions of immigrants had emigrated from Mexico, the Caribbean, and India. Generational status refers to the place of birth of a specific person or that person’s parents. For instance, first generation refers to someone who is born outside of their place of residence. Second generation refers to a person that has at least one parent that is foreign-born.
Considering the number of immigrant communities, there are often barriers that affect interactions with social structures and institutions. The complex organization of the United States healthcare system is starkly different from those of most other nations, and this may present a barrier to use for immigrants. Language barriers may also make it difficult for immigrants to access healthcare or to take control of their healthcare decisions; telephone translation services have been created to help facilitate the conversation between clinician and patient. Racial and ethnic identity may be more apparent in first-generation immigrants, and the biases and prejudices against certain racial and ethnic groups might be compounded by the individual’s immigrant status; this interplay between multiple demographic factors—especially when it leads to discrimination or oppression—is termed intersectionality. Finally, undocumented status presents a major barrier for many immigrants to access healthcare for fear of reporting and deportation.
Demographic Shifts and Social Change
Since 1950, the United States population has roughly doubled. In addition to increasing in size, the makeup of the American population has changed significantly. The average age in the United States has increased, and the population is continuing to become more racially and ethnically diverse. These are examples of demographic shifts: changes in the makeup of a population over time. These shifts can be measured by considering the population density, which counts the number of people per square kilometer of land area.
Population projections attempt to predict changes in population size over time, and can be assisted by historical measures of growth, understanding of changes in social structure, and analysis of other demographic information. To aid in the construction of population projections, population pyramids provide a histogram of the population size of various age cohorts, as shown in Figure 11.7.
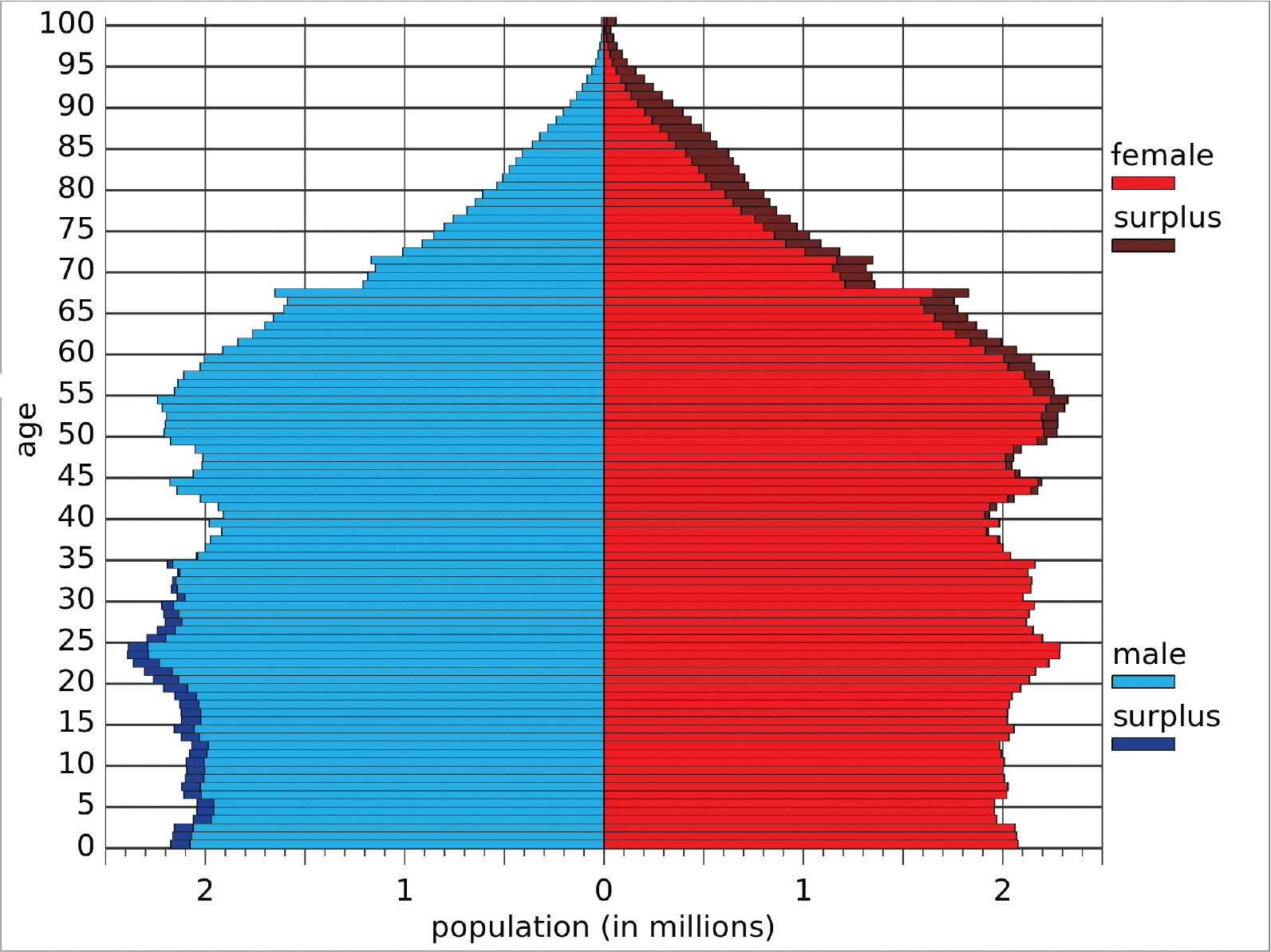
Figure 11.7 U.S. Population Pyramid, 2014 Surplus occurs when one gender has a larger population than another.
Fertility, Mortality, and Migration
The increased population of the United States is due to a number of factors that center around fertility, mortality, and migration. Fertility rate refers to the average number of children born to a woman over a lifetime in a population. In many parts of the world, fertility rate is the primary driver of population expansion; for example, in some parts of Africa, the average fertility rate is between four and eight children per woman, as seen in Figure 11.8. In the United States, fertility rates have trended downward over time; in 2013, the rate was still above two, indicating that fertility rates were still contributing to population growth.
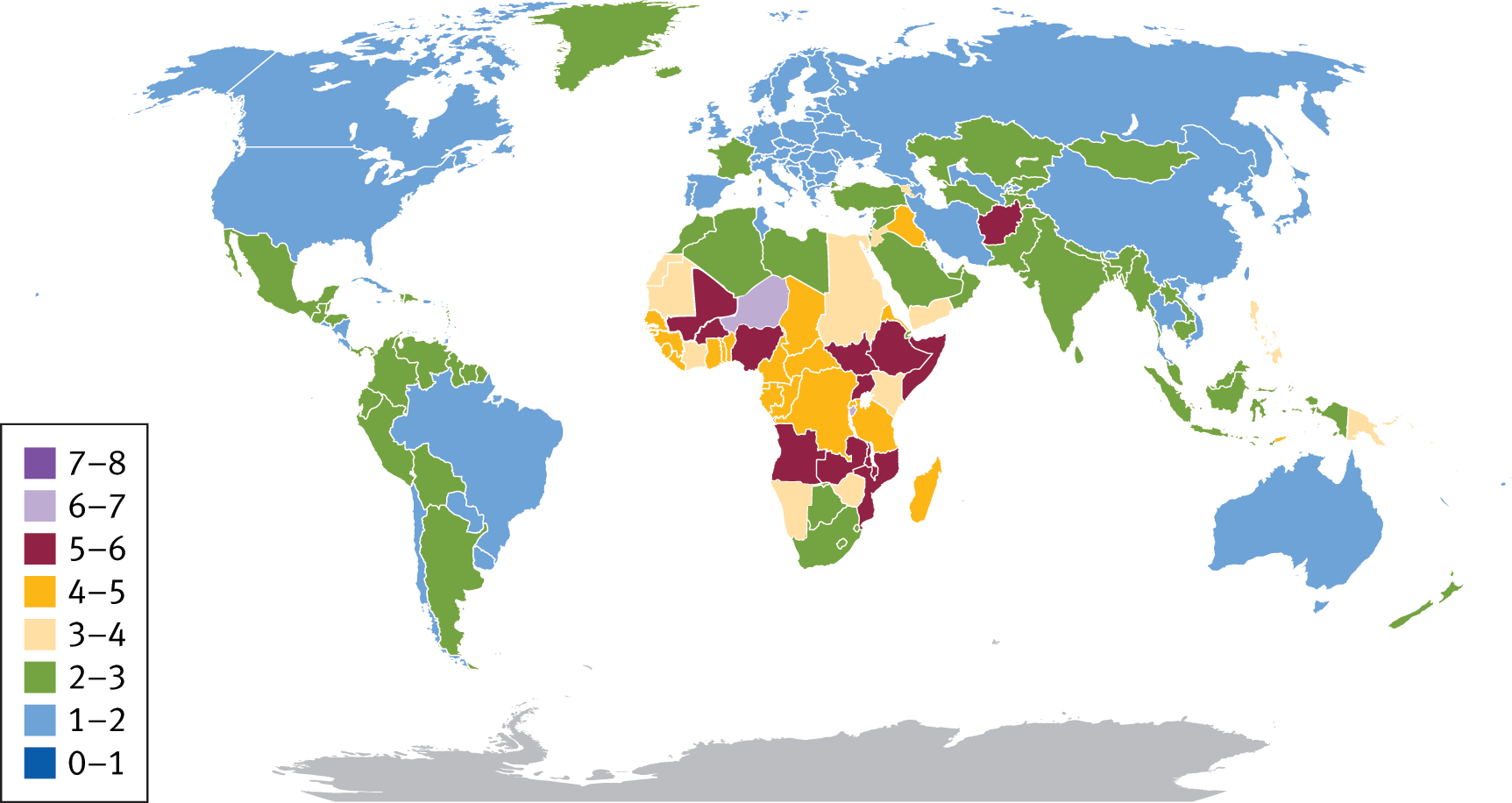
Figure 11.8 Fertility Rates around the World, 2013 Based on data from the CIA World Factbook; measured in children born per woman in the population
KEY CONCEPT
Demographic statistics:
- Fertility rate = children per woman per lifetime
- Birth rate = children per 1000 people per year
- Mortality rate = deaths per 1000 people per year
- Migration rate = immigration rate minus emigration rate
Mortality rates refer to the number of deaths in a population per unit time. Usually, this rate is measured in deaths per 1000 people per year. With advancements in healthcare and access, the mortality rate in the United States has dropped significantly over the past century. However, mortality rates are a significant brake on population growth in many parts of the world, as demonstrated in Figure 11.9. The decreased mortality rate in the United States is one contributor to the increase in average age of the population, as is a decreased fertility rate. In addition, the aging of the Baby Boomer generation, one of the largest generations in United States history, increases this average age. Both birth and mortality rates can be reported in multiple forms: the total rate for a population, the crude rate (adjusted to a certain population size over a specific period of time and multiplied by a constant to give a whole number), or age-specific rates.
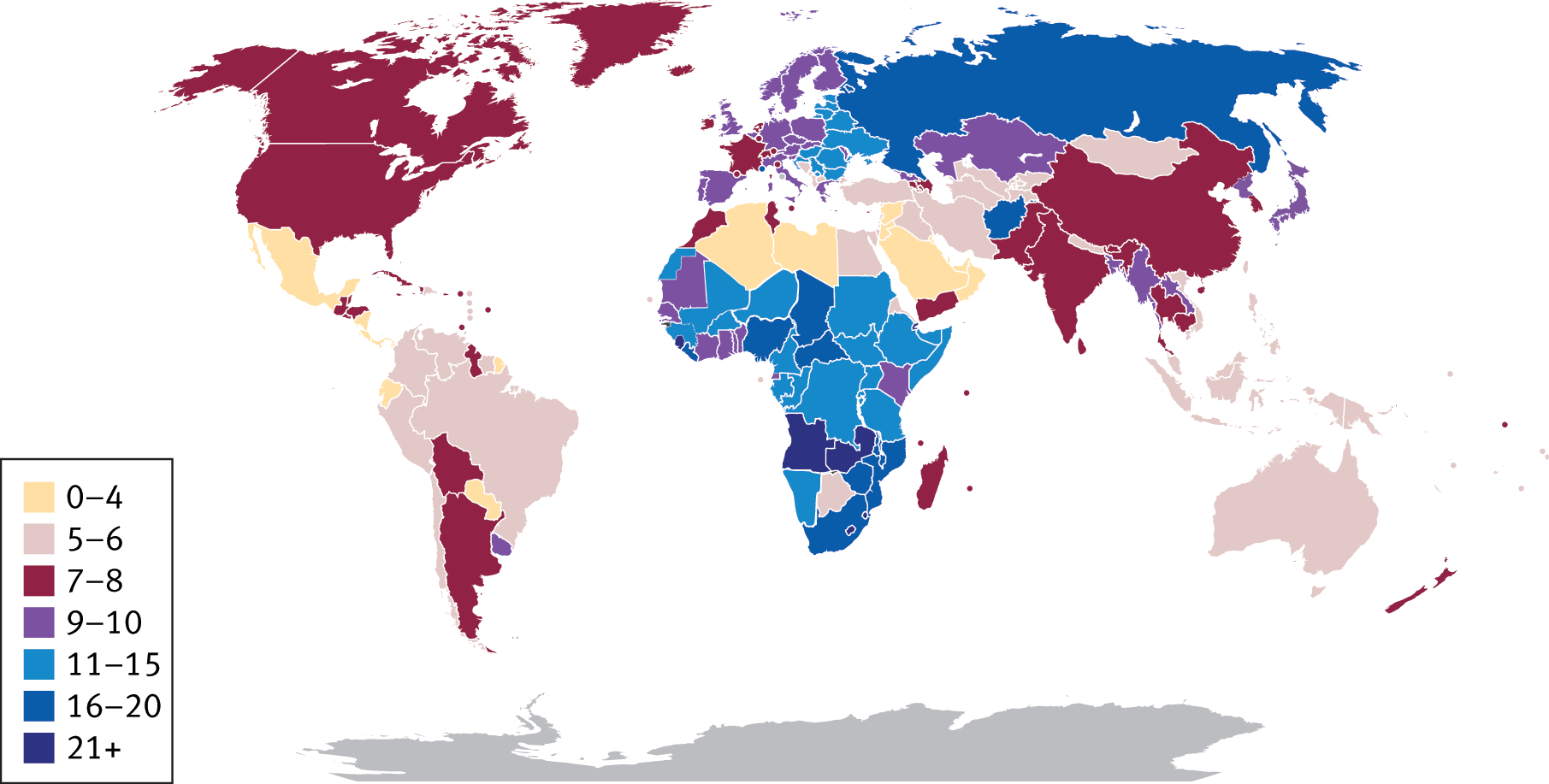
Figure 11.9. Mortality Rates around the World, 2009 Based on data from the CIA World Factbook; measured in deaths per 1000 individuals per year
Finally, migration is a contributor to population growth. Immigration is defined as movement into a new geographic space, whereas emigration is movement away from a geographic space. As described earlier, the United States continues to have larger net immigration than emigration, driving an increase in the population size. Immigration also increases the racial and ethnic diversity of the United States, as do increased mobility within the country and increases in intermarriage between different races and ethnicities. Migration can be motivated by both pull factors, which are positive attributes of the new location that attract new residents, and push factors, which are negative attributes of the old location that encourage existing residents to leave.
KEY CONCEPT
The United States population is getting bigger, older (average age has increased), and more diverse (through immigration, mobility, and intermarriage).
Demographic Transition Theory
While demographic shift refers to general changes in population makeup over time, demographic transition is a specific example of a demographic shift that occurs as a country develops from a preindustrial, or agrarian, society to an economy that is more centered on manufacturing, which is termed industrialization. Demographic transition has been seen in the United States since the Industrial Revolution and is currently occurring in many developing countries. Demographic transition theory explains this link between economic development and demographic shift in four stages:
- Stage 1: Preindustrial society; birth and death rates are both high, resulting in a stable population.
- Stage 2: Economic progress leads to improvements to healthcare, nutrition, sanitation, and wages, causing a decrease in death rates. Thus, total population increases.
- Stage 3: Improvements in contraception, women’s rights, and a shift from an agricultural to an industrial economy cause birth rates to drop. For example, with an industrializing society, children must go to school for many years to be productive in society and may need to be supported by parents for a longer period of time than was formerly the case. Thus families have fewer children, and birth rates drop. As birth and death rates equalize, population growth hits an inflection point and begins to level off.
- Stage 4: An industrialized society; birth and death rates are both low, resulting in a relative constant total population.
A model of demographic transition can be seen in Figure 11.10.
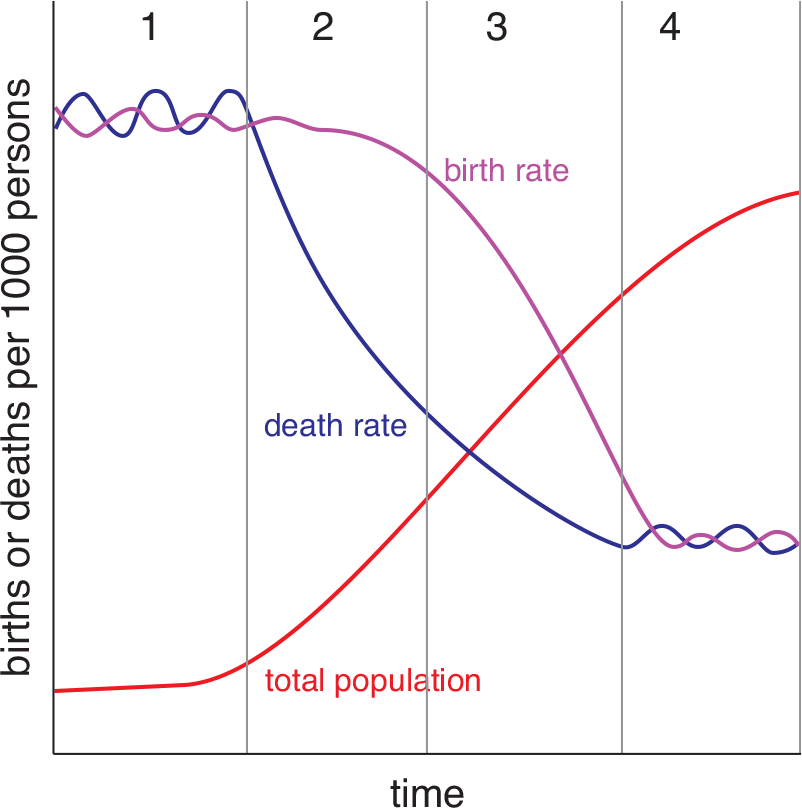
Figure 11.10. Demographic Transition
Recently, sociologists have described a fifth stage of demographic transition theory in which birth rates continue to drop and fall below the death rate, resulting in a decline of total population. Japan and Germany are currently experiencing demographic shifts expected in this theorized fifth stage.
KEY CONCEPT
During demographic transition, mortality rate drops before birth rate. Therefore, the population grows at first while mortality rate is dropping, and then plateaus as the birth rate decreases as well.
Malthusian theory focuses on how the exponential growth of a population can outpace growth of the food supply and lead to social degradation and disorder. For example, some theorists predict that demographic transition among developing nations might cause growth in the world’s population to outpace the world’s ability to generate food. The resulting hypothetical mass starvation is called the Malthusian catastrophe. This result is similar to the death phase of bacterial growth, when resources in the environment have been depleted, as described in Chapter 1 of MCAT Biology Review.
Social Movements
Social movements are organized either to promote or to resist social change. These movements are often motivated by a group’s perceived relative deprivation, which is a decrease in resources, representation, or agency relative to the whole of society, or relative to what the group is accustomed to from the past. Social movements that promote social change are termed proactive; those that resist social change are reactive. Members of social movements work to correct what they perceive as social injustices. Some examples of proactive movements include the civil rights movement, women’s rights movement, gay rights movement, animal rights movement, and environmentalism movement. Some examples of reactive movements include the White supremacist movement, counterculture movement, antiglobalization movement, and anti-immigration movement. To further their goals, social movements may establish coordinated organizations. Social movements may also seek to use different methods for driving forward their goals. The theory of resource mobilization considers how groups involved in social movements successfully achieve their objectives through the utilization and collection of resources, such as money, attention, skills, or materials. For example, in addition to coordinating cooperation between different groups, social movements may also seek to increase their audience by sharing their message through social media, which in turn can lead to increased support and more donations. Political involvement is also common through lobbying and donations, where the hope is to gain political favor that aids in the support of the group and their goals.
Globalization
Globalization is the process of merging of the separate nations of the world into a single sociocultural entity, and is a relatively recent phenomenon spurred on by improvements in global communication technology and economic interdependence. Globalization leads to a decrease in the geographical constraints on social and cultural exchanges and can lead to both positive and negative effects. For example, the availability of foods (especially produce) from around the world during the entire calendar year can only be accomplished through trade with an extremely large number of world markets. However, significant worldwide unemployment, rising prices, increased pollution, civil unrest (particularly in unindustrialized or undemocratic nations), and global terrorism are negative effects of globalization.
Traditionally, the health sector has been organized at the national, state, or local level, but this is beginning to change. Groups such as the World Health Organization (WHO), the American Red Cross, and Doctors Without Borders supply aid to populations in need around the globe. Many medical schools are also increasing opportunities for medical students to complete rotations in other countries.
Urbanization
Urbanization refers to dense areas of population creating a pull for migration. In other words, cities are formed as individuals move into and establish residency in these new urban centers. Urbanization is not a new phenomenon; ancient populations established cities in Jerusalem, Athens, Timbuktu, and other locations. The economic opportunities offered in cities and creation of a large number of “world cities” has fueled an increase in urbanization during the last few decades. Currently, more than half of the world’s populations live in what are considered urban areas. Sociologists and other professionals have found links between urban societies and health challenges related to water sanitation, air quality, environmental hazards, violence and injuries, infectious diseases, unhealthy diets, and physical inactivity.
Cities are rarely homogenous with respect to their population makeup. Most cities have areas that are more socioeconomically well-off and others that are more impoverished. Sometimes, members of specific racial, ethnic, or religious groups are concentrated in particular areas, usually due to social or economic inequities. In the most extreme cases, as shown in Figure 11.11, there arises an extremely densely populated area of a city with low-quality, often informal housing and poor sanitation.

Figure 11.11. A Disadvantaged Area in Jakarta, Indonesia
MCAT CONCEPT CHECK 11.3
Before you move on, assess your understanding of the material with these questions.
_________________________
- What is the difference between race and ethnicity?
_________________________
- What is symbolic ethnicity?
- Define the following demographic statistics:
________________________________
- Fertility rate:
________________________________
- Birth rate:
_________________________
- Mortality rate:
- During demographic transition, what happens to the mortality rate? To the birth rate?
________________________________
- Mortality rate:
_________________________
- Birth rate:
- What are the two types of social movements? How do they differ?
- _________________________
- _________________________
Conclusion
There are three major trends that are changing our nation’s healthcare needs and our patient population. First, the increased diversity in the American population as a whole (from immigration, increased social and academic mobility, and interconnectedness through technology) puts us in front of patients whose thoughts and beliefs about health and well-being may be starkly different from our own. Second, increased access to healthcare through reform legislation has allowed millions of Americans to reach providers for the first time. Finally, our successes in medicine and public health have increased survival rates of many formerly fatal conditions and have enabled us to live longer. This leaves us with an aging population, in which individuals may be coping with multiple illnesses simultaneously.
To arm physicians of the future with the skills needed to take care of this population, many medical schools are increasing their coursework in interpersonal skills (Doctor–Patient Relationship; Doctoring; or Physician, Patient, and Society are such courses at various schools), as well as cultural sensitivity, the recognition and respect of differences between cultures, and research ethics. This is part of the biopsychosocial model of medicine described in Chapter 7 of MCAT Behavioral Sciences Review. Knowledge of the structure of society and how it shifts over time, as explained in this chapter, will enhance your ability to communicate with patients. Unlike the old model of doctor knows best (often referred to as the paternalistic approach to medicine), today’s doctors must work together with patients to find solutions to their health problems. By working with patients on their own terms, you will be able to help maintain and improve their health status and begin to correct the health inequities that exist in today’s population. In the next chapter—the last of MCAT Behavioral Sciences Review—we will explore these inequities in resources, health status, and healthcare.
GO ONLINE
You’ve reviewed the content, now test your knowledge and critical thinking skills by completing a test-like passage set in your online resources!
CONCEPT SUMMARY
Sociology: Theories and Institutions
- Theoretical approaches provide frameworks for the interactions we observe within society.
- Functionalism focuses on the function of each component of society and how those components fit together. Manifest functions are deliberate actions that serve to help a given system; latent functions are unexpected, unintended, or unrecognized positive consequences of manifest functions.
- Conflict theory focuses on how power differentials are created and how these differentials contribute to the maintenance of social order.
- Symbolic interactionism is the study of the ways individuals interact through a shared understanding of words, gestures, and other symbols.
- Social constructionism explores the ways in which individuals and groups make decisions to agree upon a given social reality.
- Rational choice theory states that individuals will make decisions that maximize potential benefit and minimize potential harm; exchange theory applies rational choice theory within social groups.
- Feminist theory critiques the institutional power structures that disadvantage women in society.
- Social institutions are well-established social structures that dictate certain patterns of behavior or relationships and are accepted as a fundamental part of culture. Common social institutions include the family, education, religion, government and the economy, and health and medicine.
- There are four key ethical tenets of American medicine.
- Beneficence refers to acting in the patient’s best interest.
- Nonmaleficence refers to avoiding treatments for which risk is larger than benefit.
- Respect for autonomy refers to respecting patients’ rights to make decisions about their own healthcare.
- Justice refers to treating similar patients similarly and distributing healthcare resources fairly.
Culture
- Culture encompasses the lifestyle of a group of people and includes both material and symbolic elements.
- Material culture includes the physical items one associates with a given group, such as artwork, emblems, clothing, jewelry, foods, buildings, and tools.
- Symbolic culture includes the ideas associated with a cultural group.
- Cultural lag refers to the idea that material culture changes more quickly than symbolic culture.
- A cultural barrier is a social difference that impedes interaction.
- Language consists of spoken, signed, or written symbols combined into a system and governed by rules.
- A value is what a person deems important in life.
- A belief is something a person considers to be true.
- A ritual is a formalized ceremonial behavior in which members of a group or community regularly engage. It is governed by specific rules, including appropriate behavior and a predetermined order of events.
- Norms are societal rules that define the boundaries of acceptable behavior.
- There is evidence that culture flows from evolutionary principles, and that culture can also influence evolution.
Demographics
- Demographics refer to the statistics of populations and are the mathematical applications of sociology. One can analyze hundreds of demographic variables; some of the most common are age, gender, race and ethnicity, sexual orientation, and immigration status.
- Ageism is prejudice or discrimination on the basis of a person’s age.
- Gender is the set of behavioral, cultural, or psychological traits typically associated with a biological sex. Gender inequality is the intentional or unintentional empowerment of one gender to the detriment of the other.
- Race is a social construct based on phenotypic differences between groups of people; these may be either real or perceived differences.
- Ethnicity is also a social construct that sorts people by cultural factors, including language, nationality, religion, and other factors. Symbolic ethnicity is recognition of an ethnic identity that is only relevant on special occasions or in specific circumstances and does not specifically impact everyday life.
- Sexual orientation can be defined by one’s sexual interest toward members of same or different genders.
- Immigration is the movement into a new geographic area. Emigration is the movement away from a geographic area.
- A fertility rate is the average number of children born to a woman over a lifetime in a population. A birth rate is relative to a population size over time, usually measured as the number of births per 1000 people per year.
- A mortality rate is the average number of deaths per population size over time, usually measured as the number of deaths per 1000 people per year.
- Migration refers to the movement of people from one geographic location to another.
- Demographic transition is a model used to represent drops in birth and death rates as a result of industrialization.
- Social movements are organized to either promote (proactive) or resist (reactive) social change.
- Globalization is the process of integrating a global economy with free trade and tapping of foreign labor markets.
- Urbanization refers to the process of dense areas of population creating a pull for migration or, in other words, creating cities.
ANSWERS TO CONCEPT CHECKS
**11.1**
- Manifest functions are actions that are intended to help some part of a system. Latent functions are unintended, unstated, or unrecognized positive consequences of these actions on society.
-
Theoretical Approach Primary Thesis or Idea Functionalism Each part of society serves a function; when these functions work together correctly, society overall can function normally
Conflict theory Power differentials are created when groups compete for economic, social, and political resources; these differentials contribute to the maintenance of social order
Symbolic interactionism Humans communicate through words, gestures, and other symbols to which we attach meaning
Social constructionism Individuals and groups make decisions to agree upon a given social reality
Rational choice theory Individuals will make decisions that maximize potential benefit and minimize potential harm
Feminist theory Critiques the institutional power structures that disadvantage women in society
-
Ethical Principle Description Beneficence Act in the patient’s best interest
Nonmaleficence Do no harm; avoid interventions where the potential for harm outweighs the potential for benefit
Respect for autonomy Respect patients’ decisions and choices about their own healthcare
Justice Treat similar patients with similar care; distribute healthcare resources fairly
**11.2**
- Material culture focuses on the artifacts associated with a group: the physical objects, such as artwork, emblems, clothing, jewelry, foods, buildings, and tools. Symbolic culture focuses on the ideas and principles that belong to a particular group.
- A value is what a person deems to be important; a belief is what a person deems to be true. While these terms are often used interchangeably in everyday life, they have specific definitions in the social sciences.
**11.3**
- Race is based on phenotypic differences between groups of people. Ethnicity is based on common language, religion, nationality, or other cultural factors.
- Symbolic ethnicity is recognition of an ethnic identity on special occasions or in specific circumstances, but not during everyday life.
- Fertility rate is the average number of children a woman has over a lifetime in a population. Birth rate is the number of births in a population per unit time, usually measured as births per 1000 people per year. Mortality rate is the number of deaths in a population per unit time, usually measured as deaths per 1000 people per year.
- During demographic transition, both the mortality and birth rates decrease.
- Proactive social movements are in favor of a specific social change. Reactive social movements run against a specific social change.
SCIENCE MASTERY ASSESSMENT EXPLANATIONS
1. A
A manifest function is an intended positive effect on a system. A latent function is an unintended positive effect on a system, (C). A negative effect on a system, (B) and (D), is termed a dysfunction.
2. C
Symbolic interactionism studies how individuals interact through a shared understanding of words, gestures, and other symbols. A nod is thus a symbol in many cultures that signifies “yes.”
3. D
The principle of nonmaleficence states that physicians must not only act in their patient’s best interest (beneficence, (B)), but must also avoid treatments where the potential for harm outweighs the potential for benefit.
4. C
Although one’s dominant physical features are associated with race, this man’s preferences are those of Latino ethnicity and culture. Ethnicity is a social construct that considers language, religion, nationality, and cultural factors. Culture relates to a group’s way of life; the preferences listed in the question are examples of material and symbolic culture.
5. D
In the United States, it is not a common practice to say, “I love you,” and hug one’s physician after each routine checkup; therefore, this behavior could be considered deviant, going against the social norm. Values, (C), are what an individual deems to be important.
6. B
Both birth rate and mortality rate can be measured per 1000 people per year. Fertility rate is measured in number of children per woman over a lifetime.
7. B
Rituals are formalized ceremonial behaviors in which members of a group or community regularly engage. Therefore, these activities are examples of rituals performed for healing.
8. A
With a decrease in mortality rate and a higher immigration rate than emigration rate, the United States population continues to grow, with an increasing average age and increasing racial and ethnic diversity.
9. C
Material culture includes any cultural artifact—an object to which meaning is assigned. Values are ideas, which are associated with symbolic culture.
10. D
During demographic transition, both birth rates and mortality rates are high in stage 1, (A). Mortality rates drop during stage 2, (B), and then birth rates drop during stage 3, (C). In stage 4, both birth rates and mortality rates are low.
11. D
In this scenario, a group is fighting for social power, which is an aspect of conflict theory. Further, this group is an example of a reactive social movement because it is running counter to social change. The fact that gambling had been legalized implies the involvement of the government, a social institution.
12. C
This man is describing his sexuality as mostly homosexual, although he has also had some heterosexual attractions. The Kinsey scale scores a 6, (D), as exclusively homosexual. A score of 3 would equate to bisexuality. Thus, this man would likely score a 4 or 5.
13. B
Sex is determined by one’s genotype, and therefore is biologically determined. Gender, (A), may or may not match biological sex and therefore is not biologically determined. Ethnicity, (C), is a social construct that sorts people by cultural factors, and therefore is not biologically determined. Sexual orientation, (D), may have some biological component, but the relative role of biology and environment is not yet known.
14. B
If the immigration rate in a geographic area is larger than the emigration rate, then there is a larger influx than efflux of people. This will increase the population of that area.
15. A
Urbanization is the migration of people into urban centers to create cities. The increased population density should provide additional opportunities for social interaction, not decreased opportunities.
GO ONLINE
Consult your online resources for additional practice.
SHARED CONCEPTS
Behavioral Sciences Chapter 6
Identity and Personality
Behavioral Sciences Chapter 8
Social Processes, Attitudes, and Behavior
Behavioral Sciences Chapter 9
Social Interaction
Behavioral Sciences Chapter 10
Social Thinking
Behavioral Sciences Chapter 12
Social Stratification
Biology Chapter 12
Genetics and Evolution