Chemical Control of the Brain and Behavior
BOX 15.1 OF SPECIAL INTEREST: Stress and the Brain
Neurotransmitters and the Pharmacology of Autonomic Function
Anatomy and Functions of the Diffuse Modulatory Systems
BOX 15.2 OF SPECIAL INTEREST: You Eat What You Are
BOX 15.3 PATH OF DISCOVERY: Exploring the Central Noradrenergic Neurons, by Floyd Bloom
The Dopaminergic Substantia Nigra and Ventral Tegmental Area
The Cholinergic Basal Forebrain and Brain Stem Complexes
It should be obvious by now that knowing the organization of synaptic connections is essential to understanding how the brain works. It’s not from a love of Greek and Latin that we belabor neuroanatomy! Most of the connections we have described are precise and specific. For example, for you to be able to read these words, there must be a very fine-grained neural mapping of the light falling on your retina—how else could you see the dot in this question mark? The information must be carried centrally and dispersed precisely to many parts of the brain for processing, coordinated with control of the motor neurons that closely regulate the six muscles of each eye as it scans the page.
In addition to anatomical precision, point-to-point communication in the sensory and motor systems requires mechanisms that restrict synaptic communication to the cleft between the axon terminal and its target. It just wouldn’t do for glutamate released in the somatosensory cortex to activate neurons in the motor cortex! Furthermore, transmission must be brief enough to allow rapid responses to new sensory inputs. Thus, at these synapses, only minute quantities of neurotransmitter are released with each impulse, and these molecules are then quickly destroyed enzymatically or taken up by neighboring cells. The postsynaptic actions at transmitter-gated ion channels last only as long as the transmitter is in the cleft, a few milliseconds at most. Many axon terminals also possess presynaptic “autoreceptors” that detect the transmitter concentrations in the cleft and inhibit release if they get too high. These mechanisms ensure that this type of synaptic transmission is tightly constrained, in both space and time.
The elaborate mechanisms that constrain point-to-point synaptic transmission are somewhat like those in telecommunications. Telephone systems make possible very specific connections between one place and another so that your mother in Tacoma can talk just to you in Providence, reminding you that her birthday was last week. The telephone lines or cellular transmissions act like precise synaptic connections. The influence of one neuron (your mother) is targeted to a small number of other neurons (in this case, only you). The embarrassing message is limited to your ears only. The influence of a neuron in one of the sensory or motor systems discussed so far usually extends to the few dozen or few hundred cells it synapses on—a conference call, to be sure, but still relatively specific.
Now imagine your mother being interviewed on a television talk show broadcast on a satellite network. The widespread satellite transmission may allow her to tell millions of people that you forgot her birthday, and the loudspeaker in each television set will announce the message to anyone within earshot. Likewise, certain neurons communicate with hundreds of thousands of other cells. These widespread systems tend to act relatively slowly, over seconds to minutes. Because of their broad, protracted actions, such systems in the brain can orchestrate entire behaviors, ranging from falling asleep to falling in love. Indeed, many of the behavioral dysfunctions collectively known as mental disorders are believed to result specifically from imbalances of certain of these chemicals.
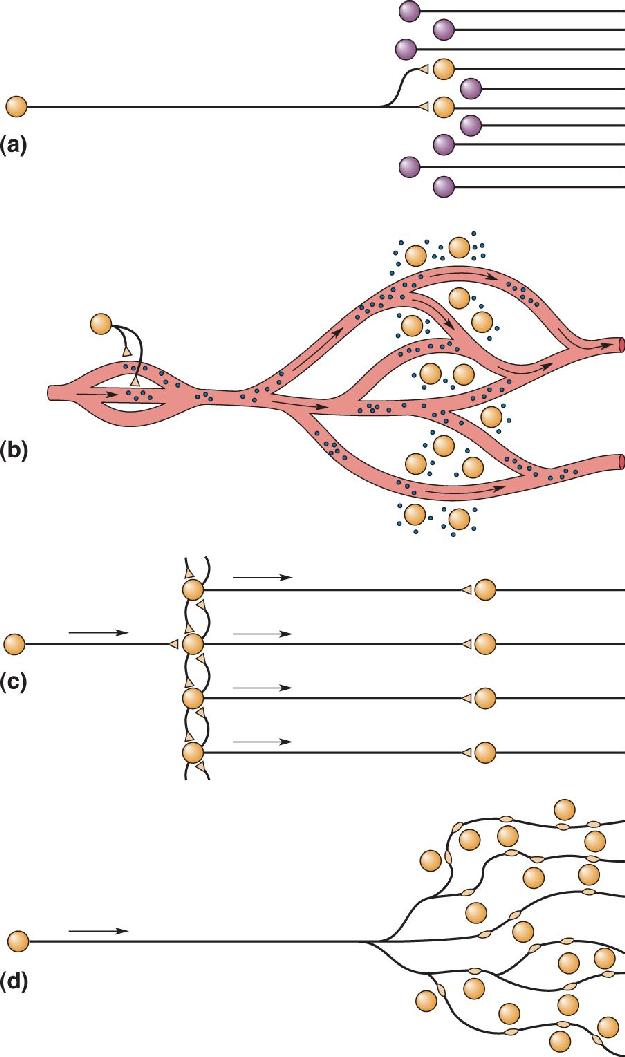
In this chapter, we look at three components of the nervous system that operate in expanded space and time (Figure 15.1). One component is the secretory hypothalamus. By secreting chemicals directly into the bloodstream, the secretory hypothalamus can influence functions throughout both the brain and the body. A second component, controlled neurally by the hypothalamus, is the autonomic nervous system (ANS), introduced in Chapter 7. Through extensive interconnections within the body, the ANS simultaneously controls the responses of many internal organs, blood vessels, and glands. The third component exists entirely within the central nervous system (CNS) and consists of several related cell groups that differ with respect to the neurotransmitter they use. All of these cell groups extend their spatial reach with highly divergent axonal projections and prolong their actions by using metabotropic postsynaptic receptors. Members of this component of the nervous system are called the diffuse modulatory systems of the brain. The diffuse systems are believed to regulate, among other things, the level of arousal and mood.

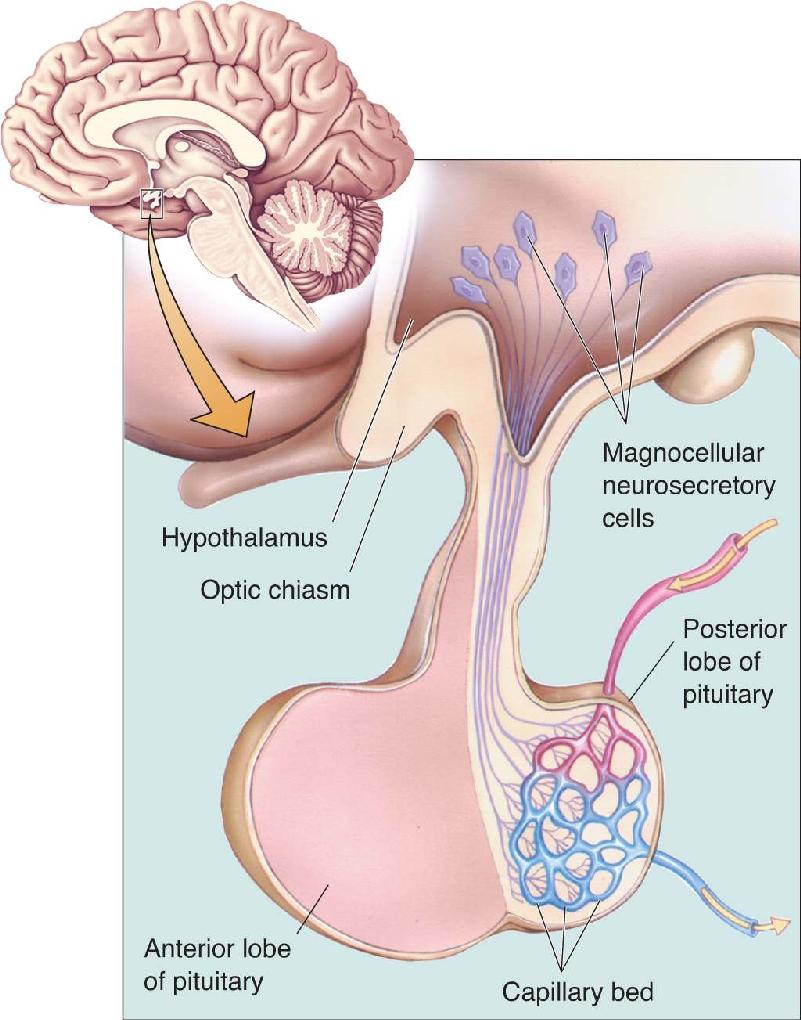
FIGURE 15.1 Patterns of communication in the nervous system. (a) Most of the systems we have discussed in this book may be described as point-to-point. The proper functioning of these systems requires restricted synaptic activation of target cells and signals of brief duration. In contrast, three other components of the nervous system act over great distances and for long periods of time. (b) Neurons of the secretory hypothalamus affect their many targets by releasing hormones directly into the bloodstream. (c) Networks of interconnected neurons of the ANS can work together to activate tissues all over the body. (d) Diffuse modulatory systems extend their reach with widely divergent axonal projections. Description
This chapter serves as a general introduction to these systems. Later chapters will explore how they contribute to specific behaviors and brain states: motivation (Chapter 16), sexual behavior (Chapter 17), emotion (Chapter 18), sleep (Chapter 19), and psychiatric disorders (Chapter 22).
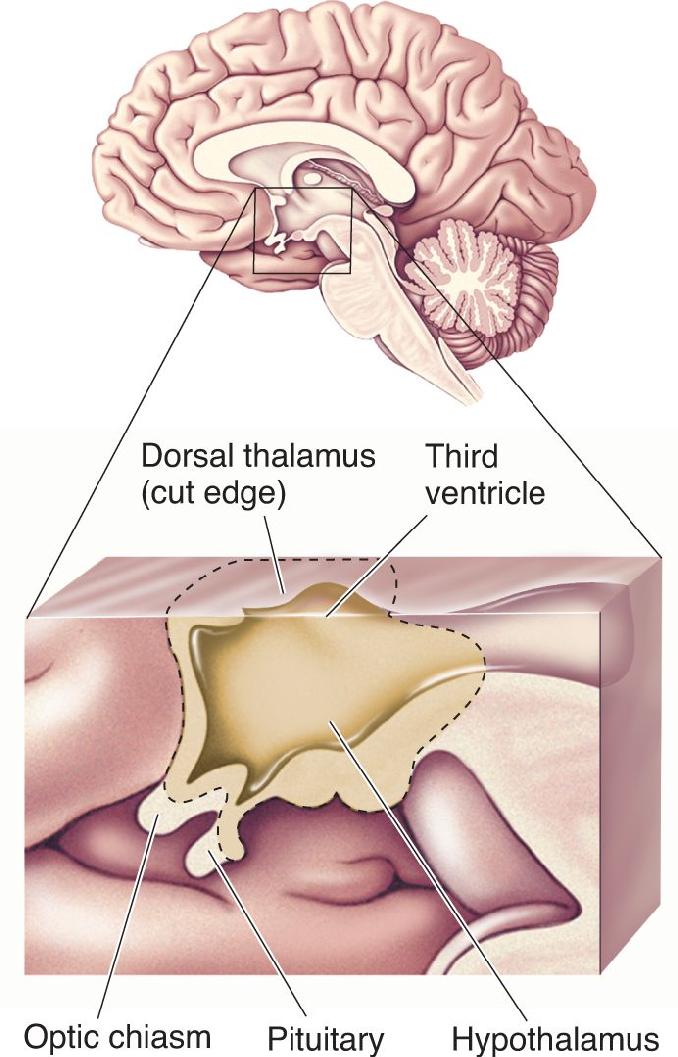
Recall from Chapter 7 that the hypothalamus sits below the thalamus, along the walls of the third ventricle. It is connected by a stalk to the pituitary gland, which dangles below the base of the brain, just above the roof of your mouth (Figure 15.2). Although this tiny cluster of nuclei makes up less than 1% of the brain’s mass, the influence of the hypothalamus on body physiology is enormous. Let’s take a brief tour of the hypothalamus and then focus on some of the ways in which it exerts its powerful influence.

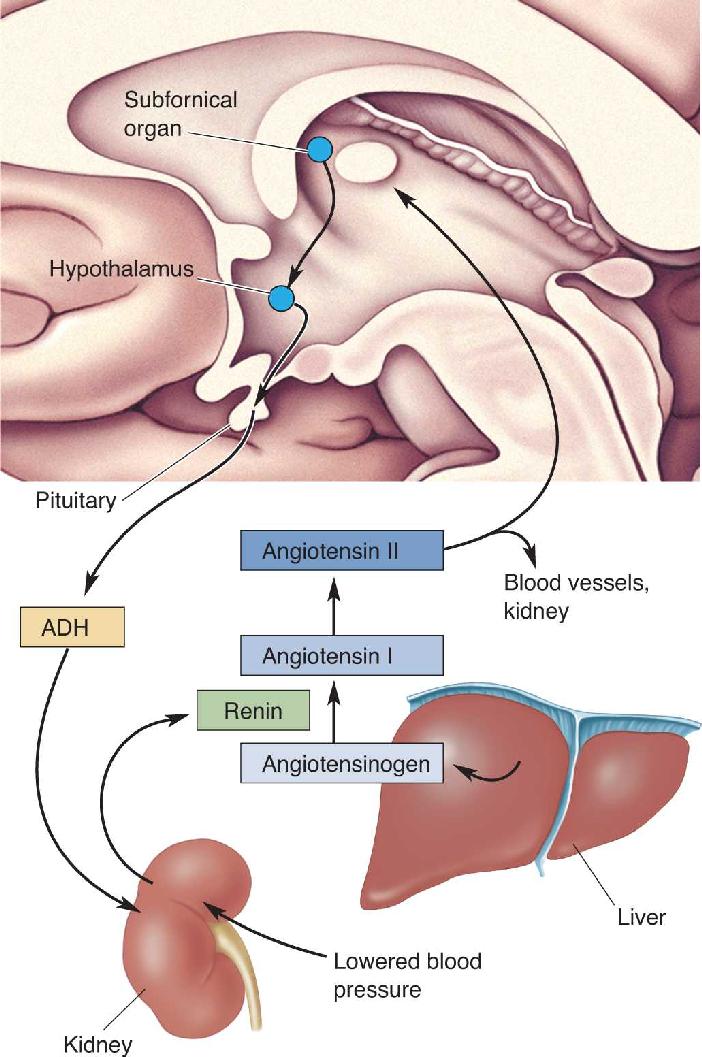
FIGURE 15.2 Locations of the hypothalamus and pituitary. This is a midsagittal section. Notice that the hypothalamus, whose borders are indicated with a dashed line, forms the wall of the third ventricle and sits below the dorsal thalamus. Description
The hypothalamus and dorsal thalamus are adjacent to one another, but their functions are very different. As we saw in the previous seven chapters, the dorsal thalamus lies in the path of all the point-to-point pathways whose destination is the neocortex. Accordingly, the destruction of a small part of the dorsal thalamus can produce a discrete sensory or motor deficit, such as a little blind spot or a lack of feeling on a portion of skin. In contrast, the hypothalamus integrates somatic and visceral responses in accordance with the needs of the brain. A tiny lesion in the hypothalamus can produce dramatic and often fatal disruptions of widely dispersed bodily functions.
Homeostasis. In mammals, the requirements for life include a narrow range of body temperatures and blood compositions. The hypothalamus regulates these levels in response to a changing external environment. This regulatory process is called homeostasis, the maintenance of the body’s internal environment within a narrow physiological range.
Consider temperature regulation. Biochemical reactions in many cells of the body are fine-tuned to occur at about 37 °C. A deviation of more than a few degrees in either direction can be catastrophic. Temperature-sensitive cells in the hypothalamus detect changes in brain temperature and orchestrate the appropriate responses. For example, if you stroll naked through the snow, the hypothalamus issues commands that cause you to shiver (generating heat in the muscles), develop goose bumps (a futile attempt to fluff up your nonexistent fur for better insulation—a reflexive remnant from our hairier ancestors), and turn blue (shunting blood away from cold surface tissues to keep the sensitive core of the body warmer). In contrast, when you go for a jog in the tropics, the hypothalamus activates heat-loss mechanisms that make you turn red (shunting blood to surface tissues where heat can radiate away) and sweat (cooling the skin by evaporation).
Other examples of homeostasis are the tight regulation of blood volume, pressure, salinity, acidity, and blood oxygen and glucose concentrations. The means by which the hypothalamus achieves these different types of regulation are remarkably diverse.
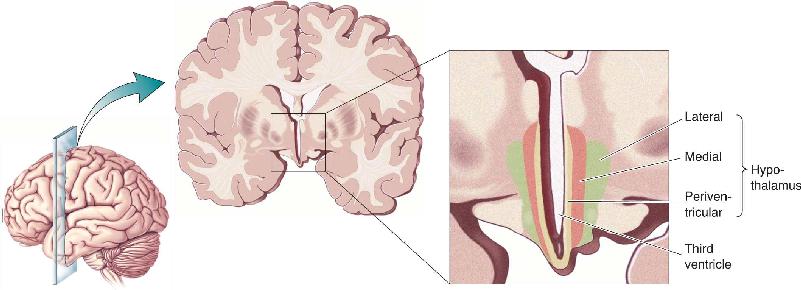
Structure and Connections of the Hypothalamus. Each side of the hypothalamus has three functional zones: lateral, medial, and periventricular (Figure 15.3). The lateral and medial zones have extensive connections with the brain stem and the telencephalon and regulate certain types of behavior, as we will see in Chapter 16. Here we are concerned only with the third zone, which actually receives much of its input from the other two.

FIGURE 15.3 Zones of the hypothalamus. The hypothalamus has three functional zones: lateral, medial, and periventricular. The periventricular zone receives inputs from the other zones, the brain stem, and the telencephalon. Neurosecretory cells in the periventricular zone secrete hormones into the bloodstream. Other periventricular cells control the autonomic nervous system.
The periventricular zone is so named because, with the exception of a thin finger of neurons that are displaced laterally by the optic tract (called the supraoptic nucleus), the cells of this region lie right next to the wall of the third ventricle. Within this zone exists a complex mix of neurons with different functions. One group of cells constitutes the suprachiasmatic nucleus (SCN), which lies just above the optic chiasm. These cells receive direct retinal innervation and function to synchronize circadian rhythms with the daily light–dark cycle (see Chapter 19). Other cells in the periventricular zone control the ANS and regulate the outflow of the sympathetic and parasympathetic innervation of the visceral organs. The cells in a third group, called neurosecretory neurons, extend axons down toward the stalk of the pituitary gland. These are the cells that now command our attention.
We have said that the pituitary dangles below the base of the brain, which is true when the brain is lifted out of the head. In a living brain, however, the pituitary is gently held in a cradle of bone at the base of the skull. It requires this special protection because it is the “mouthpiece” from which much of the hypothalamus “speaks” to the body. The pituitary has two lobes, posterior and anterior. The hypothalamus controls the two lobes in different ways.
Hypothalamic Control of the Posterior Pituitary. The largest of the hypothalamic neurosecretory cells, magnocellular neurosecretory cells, extend axons down the stalk of the pituitary and into the posterior lobe (Figure 15.4). In the late 1930s, Ernst and Berta Scharrer, working at the University of Frankfurt in Germany, proposed that these neurons release chemical substances directly into the capillaries of the posterior lobe. At the time, this was quite a radical idea. It was well established that chemical messengers called hormones were released by glands into the bloodstream, but no one had thought that a neuron could act like a gland or that a neurotransmitter could act like a hormone. The Scharrers were correct, however. The substances released into the blood by neurons are now called neurohormones.

FIGURE 15.4 Magnocellular neurosecretory cells of the hypothalamus. This is a midsagittal view of the hypothalamus and pituitary. Magnocellular neurosecretory cells secrete oxytocin and vasopressin directly into capillaries in the posterior lobe of the pituitary. Description
The magnocellular neurosecretory cells release two neurohormones into the bloodstream, oxytocin and vasopressin. Both of these chemicals are peptides, each consisting of a chain of nine amino acids. Oxytocin has sometimes been called the “love hormone” because levels rise during sexual or intimate behaviors and promote social bonding (discussed further in Chapter 17). In women, it also plays a critical role during the final stages of childbirth by causing the uterus to contract and facilitating the delivery of the newborn. It also stimulates the ejection of milk from the mammary glands. All lactating mothers know about the complex “letdown” reflex that involves the oxytocin neurons of the hypothalamus. Oxytocin release may be stimulated by the somatic sensations generated by a suckling baby. But the sight or sound of a baby (even someone else’s) can also trigger the release of milk beyond the mother’s conscious control. In each case, information about a sensory stimulus—somatic, visual, or auditory—reaches the cerebral cortex via the usual route, the thalamus, and the cortex ultimately stimulates the hypothalamus to trigger oxytocin release. The cortex can also suppress hypothalamic functions, such as when anxiety inhibits the letdown of milk.
Vasopressin, also called antidiuretic hormone (ADH), regulates blood volume and salt concentration. When the body is deprived of water, the blood volume decreases and blood salt concentration increases. These changes are detected by pressure receptors in the cardiovascular system and salt concentration-sensitive cells in the hypothalamus, respectively. Vasopressin-containing neurons receive information about these changes and respond by releasing vasopressin, which acts directly on the kidneys and leads to water retention and reduced urine production.
Under conditions of lowered blood volume and pressure, communication between the brain and the kidneys actually occurs in both directions (Figure 15.5). The kidneys secrete an enzyme into the blood called renin. Elevated renin sets off a sequence of biochemical reactions in the blood. Angiotensinogen, a large protein released from the liver, is converted by renin to angiotensin I, which breaks down further to form another small peptide hormone, angiotensin II. Angiotensin II has direct effects on the kidney and blood vessels, which help increase blood pressure. But angiotensin II in the blood is also detected by the subfornical organ, a part of the telencephalon that lacks a blood-brain barrier. Cells in the subfornical organ project axons into the hypothalamus where they activate, among other things, the vasopressin-containing neurosecretory cells. In addition, the subfornical organ activates cells in the lateral area of the hypothalamus, somehow producing an overwhelming thirst that motivates drinking behavior. It may be difficult to accept, but it’s true: To a limited extent, our brain is controlled by our kidneys! This example also illustrates that the means by which the hypothalamus maintains homeostasis go beyond control of the visceral organs and can include behavioral responses. In Chapter 16, we will explore in more detail how the hypothalamus incites behavior.

FIGURE 15.5 Communication between the kidneys and the brain. Under conditions of lowered blood volume or pressure, the kidney secretes renin into the bloodstream. Renin in the blood promotes the synthesis of the peptide angiotensin II, which excites the neurons in the subfornical organ. The subfornical neurons stimulate the hypothalamus, causing an increase in vasopressin (ADH) production and a feeling of thirst. Description
Hypothalamic Control of the Anterior Pituitary. Unlike the posterior lobe, which really is a part of the brain, the anterior lobe of the pituitary is an actual gland. The cells of the anterior lobe synthesize and secrete a wide range of hormones that regulate secretions from other glands throughout the body (together constituting the endocrine system). The pituitary hormones act on the gonads, the thyroid glands, the adrenal glands, and the mammary glands (Table 15.1). For this reason, the anterior pituitary was traditionally described as the body’s “master gland.” But what controls the anterior pituitary? The secretory hypothalamus. The hypothalamus itself is the true master gland of the endocrine system.
Thyroid-stimulating hormone (TSH); also called thyrotropin
Adrenocorticotropic hormone (ACTH); also called corticotropin
Cortisol secretion (mobilizes energy stores, inhibits immune system, other actions)
The anterior lobe is under the control of neurons in the periventricular area called parvocellular neurosecretory cells. These hypothalamic neurons do not extend axons all the way into the anterior lobe; instead, they communicate with their targets via the bloodstream (Figure 15.6). These neurons secrete what are called hypophysiotropic hormones into a uniquely specialized capillary bed at the floor of the third ventricle. These tiny blood vessels run down the stalk of the pituitary and branch in the anterior lobe. This network of blood vessels is called the hypothalamo-pituitary portal circulation. Hypophysiotropic hormones secreted by hypothalamic neurons into the portal circulation travel downstream until they bind to specific receptors on the surface of pituitary cells. Activation of these receptors causes the pituitary cells to either secrete or stop secreting hormones into the general circulation.

FIGURE 15.6 Parvocellular neurosecretory cells of the hypothalamus. Parvocellular neurosecretory cells secrete hypophysiotropic hormones into specialized capillary beds of the hypothalamo-pituitary portal circulation. These hormones travel to the anterior lobe of the pituitary, where they trigger or inhibit the release of pituitary hormones from secretory cells. Description
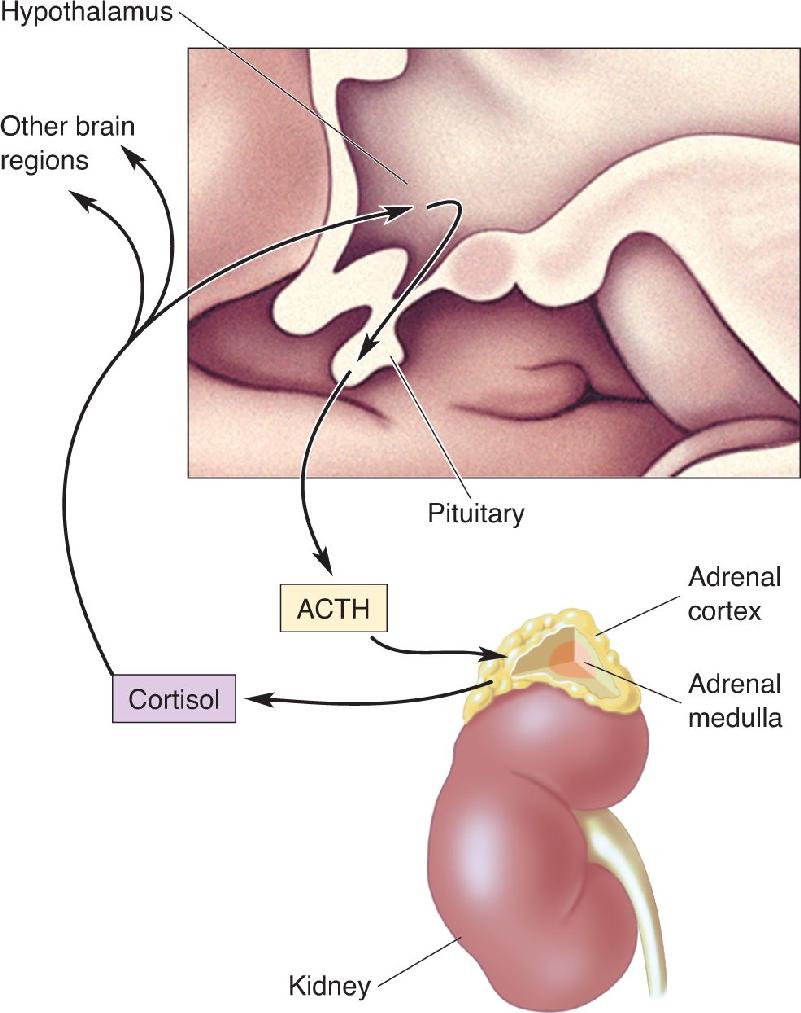
Regulation of the adrenal glands illustrates how this system works. Located just above the kidneys, the adrenal glands consist of two parts, a shell called the adrenal cortex and a center called the adrenal medulla. The adrenal cortex produces the steroid hormone cortisol; when it is released into the bloodstream, cortisol acts throughout the body to mobilize energy reserves and suppress the immune system, preparing us to carry on in the face of life’s various stresses. In fact, a good stimulus for cortisol release is stress, ranging from physiological stress, such as a loss of blood; to positive emotional stimulation, such as falling in love; to psychological stress, such as anxiety over an upcoming exam.
Parvocellular neurosecretory cells that control the adrenal cortex determine whether a stimulus is stressful or not (as defined by the release of cortisol). These neurons lie in the periventricular hypothalamus and release a peptide called corticotropin-releasing hormone (CRH) into the blood of the portal circulation. CRH travels the short distance to the anterior pituitary, where, within about 15 seconds, it stimulates the release of corticotropin, or adrenocorticotropic hormone (ACTH). ACTH enters the general circulation and travels to the adrenal cortex where, within a few minutes, it stimulates cortisol release (Figure 15.7).

FIGURE 15.7 The stress response. Under conditions of physiological, emotional, or psychological stimulation or stress, the periventricular hypothalamus secretes corticotropin-releasing hormone (CRH) into the hypothalamo-pituitary portal circulation. This triggers the release of adrenocorticotropic hormone (ACTH) into the general circulation. ACTH stimulates the release of cortisol from the adrenal cortex. Cortisol can act directly on hypothalamic neurons, as well as on other neurons elsewhere in the brain. Description
Blood levels of cortisol are, to some extent, self-regulated. Cortisol is a steroid, a class of biochemicals related to cholesterol. Thus, cortisol is a lipophilic (“fat-loving”) molecule, which dissolves easily in lipid membranes and readily crosses the blood-brain barrier. In the brain, cortisol interacts with specific receptors that lead to inhibition of CRH release, thus ensuring that circulating cortisol levels do not get too high. Physicians need to be mindful of this feedback regulation when they prescribe prednisone, a synthetic form of cortisol. Prednisone is a powerful medicine, frequently used to suppress inflammation. When administered for several days, however, the prednisone circulating in the bloodstream fools the brain into thinking that naturally released levels of cortisol are too high and shutting down the release of CRH and the adrenal cortex. Abrupt discontinuation of prednisone treatment does not give the adrenal cortex enough time to ramp up cortisol production and can thus result in what is called adrenal insufficiency. Among the symptoms of adrenal insufficiency are severe abdominal pain and diarrhea, extremely low blood pressure, and changes in mood and personality. Adrenal insufficiency is also a feature of a rare disorder called Addison’s disease, named after Thomas Addison, the British physician who first described the condition in 1849. Addison recognized that one cause of this constellation of symptoms is degeneration of the adrenal gland. Perhaps the most famous sufferer of Addison’s disease was U.S. President John F. Kennedy. Kennedy required a daily regimen of hormone replacement therapy to compensate for the loss of cortisol, a fact that was concealed during his presidency to protect his youthful and vigorous image.
The flip side of adrenal insufficiency is a condition called Cushing’s disease, caused by pituitary gland dysfunction that results in elevated levels of ACTH and, consequently, cortisol. The symptoms include rapid weight gain, immune suppression, sleeplessness, memory impairment, and irritability. Not surprisingly, the symptoms of Cushing’s disease are a common side effect of prednisone treatment. The myriad behavioral changes caused by too much (or too little) cortisol may be explained by the fact that neurons with cortisol receptors are found widely distributed in the brain, not just in the hypothalamus. In these other CNS locations, cortisol has been shown to have significant effects on neuronal activity. Thus, we see that the release of hypophysiotropic hormones by cells in the secretory hypothalamus can produce widespread alterations in the physiology of both the body and the brain (Box 15.1).
Biological stress is created by the brain in response to real or imagined stimuli. The many physiological responses associated with stress help protect the body and the brain from the dangers that triggered the stress in the first place. But stress in chronic doses can have insidious harmful effects as well. Neuroscientists have only begun to understand the relationship between stress, the brain, and brain damage.
Stress leads to the release of the steroid hormone cortisol from the adrenal cortex. Cortisol travels to the brain through the bloodstream and binds to receptors in the cytoplasm of many neurons. The activated receptors travel to the cell nucleus, where they stimulate gene transcription and ultimately protein synthesis. One consequence of cortisol’s action is that neurons admit more Ca2+ through voltage-gated ion channels. This may be due to a direct change in the channels, or it may be indirectly caused by changes in the cell’s energy metabolism. Whatever the mechanism, presumably in the short term cortisol makes the brain better able to cope with the stress—perhaps by helping it figure out a way to avoid it!
But what about the effects of chronic, unavoidable stress? In Chapter 6, we learned that too much calcium can be a bad thing. If neurons become overloaded with calcium, they die (excitotoxicity). The question naturally arises: Can cortisol kill? Bruce McEwen and his colleagues at Rockefeller University, and Robert Sapolsky and his colleagues at Stanford University, have studied this question in the rat brain. They found that daily injections of corticosterone (rat cortisol) for several weeks caused dendrites to wither in many neurons with corticosterone receptors. A few weeks later, these cells started to die. A similar result was found when, instead of daily hormone injections, the rats were stressed every day.
Sapolsky’s studies of baboons in Kenya further reveal the scourges of chronic stress. Baboons in the wild maintain a complex social hierarchy, and subordinate males steer clear of dominant males when they can. During one year when the baboon population boomed, local villagers caged many of the animals to prevent them from destroying their crops. Unable to escape the “top baboons” in the cages, many of the subordinate males subsequently died—not from wounds or malnutrition but apparently from severe and sustained stress-induced effects. They had gastric ulcers, colitis, enlarged adrenal glands, and extensive degeneration of neurons in their hippocampus. Subsequent studies suggest that it is the direct effect of cortisol that damages the hippocampus. These effects of cortisol and stress resemble the effects of aging on the brain. Indeed, research has clearly shown that chronic stress causes premature aging of the brain.
In humans, exposure to the horrors of combat, sexual abuse, and other types of extreme violence can lead to posttraumatic stress disorder, with symptoms of heightened anxiety, memory disturbances, and intrusive thoughts. Imaging studies have consistently found degenerative changes in the brains of victims, particularly in the hippocampus. In Chapter 22, we will see that stress, and the brain’s response to it, play a central role in several psychiatric disorders.
Besides controlling the ingredients of the hormonal soup that flows in our veins, the periventricular zone of the hypothalamus also controls the autonomic nervous system (ANS). The ANS is an extensive network of interconnected neurons that are widely distributed inside the body. From the Greek autonomia (roughly meaning “independence”), autonomic functions are usually carried out automatically, without conscious, voluntary control. They are also highly coordinated functions. Imagine a sudden crisis. In a morning class, as you are engrossed in a crossword puzzle, the instructor unexpectedly calls you to the blackboard to solve an impossible-looking equation. You are faced with a classic fight-or-flight situation, and your body reacts accordingly, even as your conscious mind frantically considers whether to blunder through it or beg off in humiliation. Your ANS triggers a host of physiological responses, including increased heart rate and blood pressure, depressed digestive functions, and mobilized glucose reserves. These responses are all produced by the sympathetic division of the ANS. Now imagine your relief as the class-ending bell suddenly rings, saving you from acute embarrassment and the instructor’s anger. You settle back into your chair, breathe deeply, and read the clue for 24 down. Within a few minutes, your sympathetic responses decrease to low levels, and the functions of your parasympathetic division crank up again: Your heart rate slows and blood pressure drops, digestive functions work harder on breakfast, and you stop sweating.
Notice that you may not have moved out of your chair throughout this unpleasant event. Maybe you didn’t even move your pencil. But your body’s internal workings reacted dramatically. Unlike the somatic motor system, whose alpha motor neurons can rapidly excite skeletal muscles with pinpoint accuracy, the actions of the ANS are typically multiple, widespread, and relatively slow. Therefore, the ANS operates in expanded space and time. In addition, unlike the somatic motor system, which can only excite its peripheral targets, the ANS balances synaptic excitation and inhibition to achieve widely coordinated and graded control.
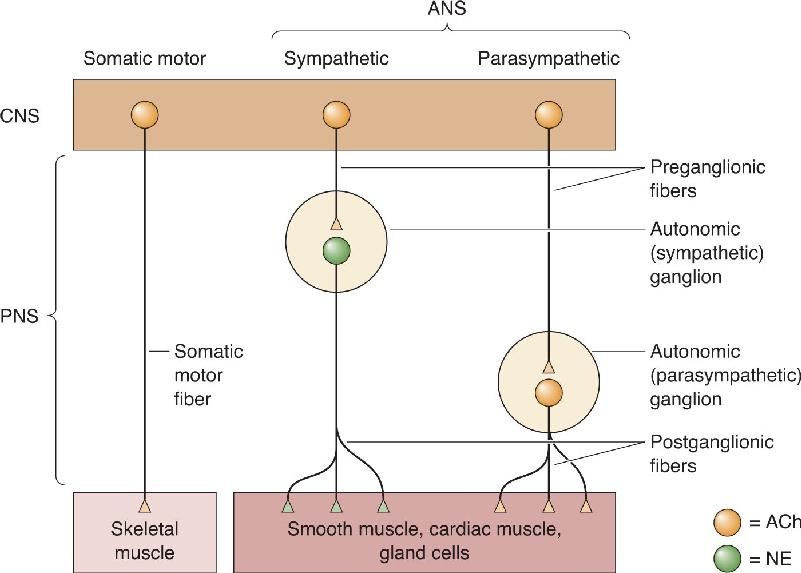
Together, the somatic motor system and the ANS constitute the total neural output of the CNS. The somatic motor system has a single function: It innervates and commands skeletal muscle fibers. The ANS has the complex task of commanding every other tissue and organ in the body that is innervated. Both systems have upper motor neurons in the brain that send commands to lower motor neurons, which actually innervate the target structures outside the nervous system. However, they have some interesting differences (Figure 15.8). The cell bodies of all somatic lower motor neurons lie within the CNS in either the ventral horn of the spinal cord or the brain stem. The cell bodies of all autonomic lower motor neurons lie outside the central nervous system, within cell clusters called autonomic ganglia. The neurons in these ganglia are called postganglionic neurons. Postganglionic neurons are driven by preganglionic neurons, whose cell bodies are in the spinal cord and brain stem. Thus, the somatic motor system controls its targets (skeletal muscles) via a monosynaptic pathway, while the ANS influences its targets (smooth muscles, cardiac muscle, and glands) using a disynaptic pathway.

FIGURE 15.8 The organization of the three neural outputs of the CNS. The sole output of the somatic motor system is the lower motor neurons in the ventral horn of the spinal cord and the brain stem, which control skeletal muscle. Visceral functions such as salivating, sweating, and genital stimulation depend on the sympathetic and parasympathetic divisions of the ANS, whose lower motor neurons (i.e., postganglionic neurons) lie outside the CNS in autonomic ganglia. Description
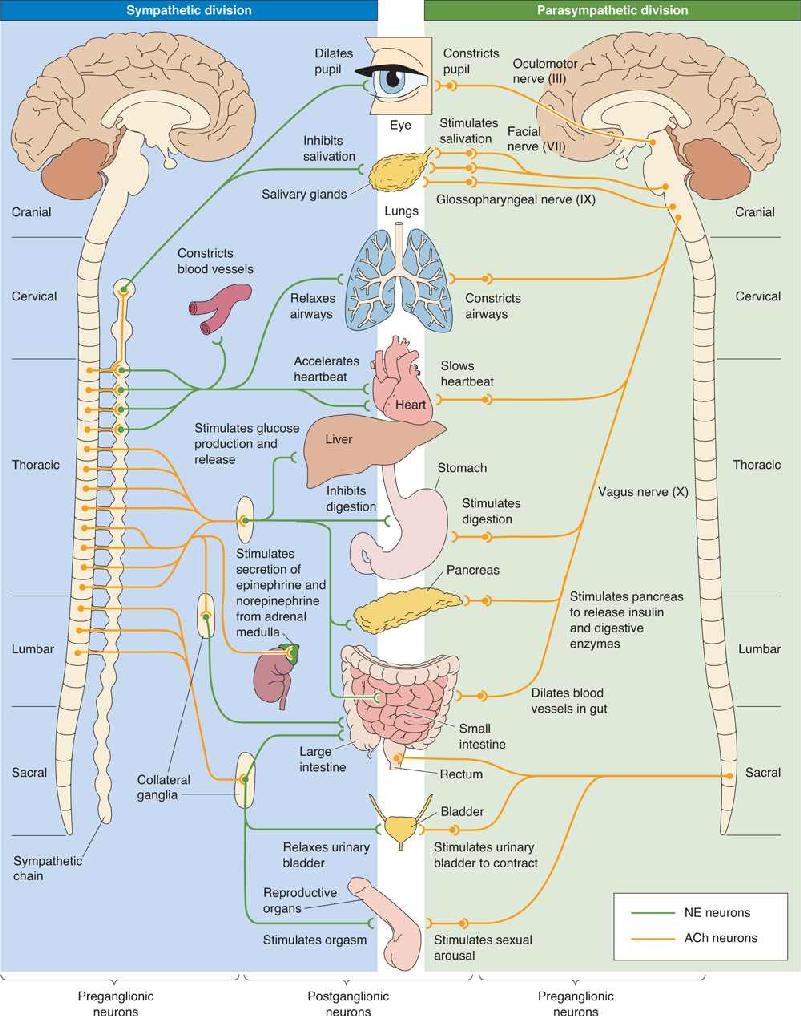
Sympathetic and Parasympathetic Divisions. The sympathetic and parasympathetic divisions operate in parallel, but they use pathways that are quite distinct in structure and in their neurotransmitter systems. Preganglionic axons of the sympathetic division emerge only from the middle third of the spinal cord (thoracic and lumbar segments). In contrast, preganglionic axons of the parasympathetic division emerge only from the brain stem and the lowest (sacral) segments of the spinal cord, so the two systems complement each other anatomically (Figure 15.9).

FIGURE 15.9 The chemical and anatomical organization of the sympathetic and parasympathetic divisions of the ANS. Notice that the preganglionic inputs of both divisions use ACh as a neurotransmitter. The postganglionic parasympathetic innervation of the visceral organs also uses ACh, but the postganglionic sympathetic innervation uses NE (with the exception of innervation of the sweat glands and vascular smooth muscle within skeletal muscle, which use ACh). The adrenal medulla receives preganglionic sympathetic innervation and secretes epinephrine into the bloodstream when activated. Note the pattern of innervation by the sympathetic division: Target organs in the chest cavity are innervated by postganglionic neurons originating in the sympathetic chain, and target organs in the abdominal cavity are innervated by postganglionic neurons originating in the collateral ganglia. Description
The preganglionic neurons of the sympathetic division lie within the intermediolateral gray matter of the spinal cord. They send their axons through the ventral roots to synapse on neurons in the ganglia of the sympathetic chain, which lies next to the spinal column, or within collateral ganglia found within the abdominal cavity. The preganglionic parasympathetic neurons, on the other hand, sit within a variety of brain stem nuclei and the lower (sacral) spinal cord, and their axons travel within several cranial nerves as well as the nerves of the sacral spinal cord. The parasympathetic preganglionic axons travel much farther than the sympathetic axons because the parasympathetic ganglia are typically located next to, on, or in their target organs (see Figures 15.8 and 15.9).
The ANS innervates three types of tissue: glands, smooth muscle, and cardiac muscle. Thus, almost every part of the body is a target of the ANS, as shown in Figure 15.9. The ANS:
- Innervates the secretory glands (salivary, sweat, tear, and various mucus-producing glands).
- Innervates the heart and blood vessels to control blood pressure and flow.
- Innervates the bronchi of the lungs to meet the oxygen demands of the body.
- Regulates the digestive and metabolic functions of the liver, gastrointestinal tract, and pancreas.
- Regulates the functions of the kidney, urinary bladder, large intestine, and rectum.
- Is essential to the sexual responses of the genitals and reproductive organs.
The physiological influences of the sympathetic and parasympathetic divisions generally oppose each other. The sympathetic division tends to be most active during a crisis, real or perceived. The behaviors related to it are summarized in the puerile (but effective) mnemonic used by medical students, called the four Fs: fight, flight, fright, and sex. The parasympathetic division facilitates various non–four-F processes, such as digestion, growth, immune responses, and energy storage. In most cases, the activity levels of the two ANS divisions are reciprocal; when one is high, the other tends to be low, and vice versa. The sympathetic division frenetically mobilizes the body for a short-term emergency at the expense of processes that keep it healthy over the long term. The parasympathetic division works calmly for the long-term good. Both cannot be stimulated strongly at the same time; their general goals are incompatible. Fortunately, neural circuits in the CNS inhibit activity in one division when the other is active.
Some examples illustrate how the balance of activity in the sympathetic and parasympathetic divisions controls organ functions. The pacemaker region of the heart triggers each heartbeat without the help of neurons, but both divisions of the ANS innervate it and modulate it; sympathetic activity results in an increase in the rate of beating, while parasympathetic activity slows it down. The smooth muscles of the gastrointestinal tract are also dually innervated, but the effect of each division is the opposite of its effect on the heart. Intestinal motility, and thus digestion, is stimulated by parasympathetic axons and inhibited by sympathetic axons. Not all tissues receive innervation from both divisions of the ANS, however. For example, blood vessels of the skin, and the sweat glands, are innervated (and excited) only by sympathetic axons. Lacrimal (tear-producing) glands are innervated (and excited) only by parasympathetic input.
Another example of the balance of parasympathetic–sympathetic activity is the curious neural control of the male sexual response. Erection of the human penis is a hydraulic process. It occurs when the penis becomes engorged with blood, which is triggered and sustained by parasympathetic activity. The curious part is that orgasm and ejaculation are triggered by sympathetic activity. You can imagine how complicated it must be for the nervous system to orchestrate the entire sexual act; parasympathetic activity gets it going (and keeps it going), but a shift to sympathetic activity is necessary to bring it to a successful conclusion. Anxiety and worry, and their attendant sympathetic activity, tend to inhibit erection and promote ejaculation. Not surprisingly, impotence and premature ejaculation are common complaints of the overstressed male. (We will discuss sexual behavior further in Chapter 17.)
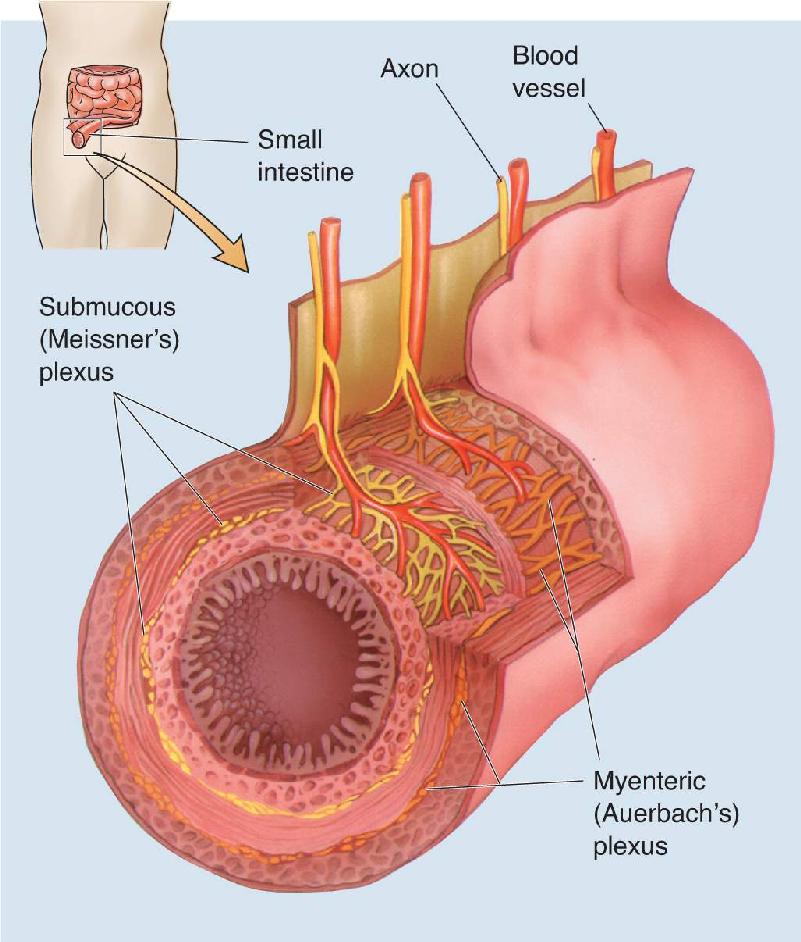
The Enteric Division. The “little brain,” as the enteric division of the ANS is sometimes called, is a unique neural system embedded in an unlikely place: the lining of the esophagus, stomach, intestines, pancreas, and gallbladder. It consists of two complicated networks, each with sensory nerves, interneurons, and autonomic motor neurons, called the myenteric (Auerbach’s) plexus and submucous (Meissner’s) plexus (Figure 15.10). These networks control many of the physiological processes involved in the transport and digestion of food, from oral to anal openings. The enteric system is not small; it contains about 500 million neurons, the same number of neurons as the entire spinal cord!

FIGURE 15.10 The enteric division of the ANS. This cross-sectional view of the small intestine shows the two networks of the enteric division: the myenteric plexus and the submucous plexus. They both contain visceral sensory and motor neurons that control the functions of the digestive organs. Description
If the enteric division of the ANS qualifies as “brain” (which may be overstating the case), it is because it can operate with a great deal of independence. Enteric sensory neurons monitor tension and stretch of the gastrointestinal walls, the chemical status of stomach and intestinal contents, and hormone levels in the blood. This information is used by enteric interneuronal circuits and motor neurons, which also reside in the gut, to govern smooth muscle motility, the production of mucous and digestive secretions, and the diameter of the local blood vessels. For example, consider a partially digested pizza making its way through the small intestine. The enteric nervous system ensures that lubricating mucus and digestive enzymes are delivered, that rhythmic (peristaltic) muscle action works to mix the pizza and enzymes thoroughly, and that intestinal blood flow increases to provide a sufficient fluid source and transport newly acquired nutrients to the rest of the body.
The enteric division is not entirely autonomous. It receives input indirectly from the “real” brain via axons of the sympathetic and parasympathetic divisions. These provide supplementary control and can supersede the functions of the enteric division in some circumstances. For example, the enteric nervous system and digestive functions are inhibited by the strong activation of the sympathetic nervous system that occurs during acute stress.
Central Control of the ANS. As we have said, the hypothalamus is the main regulator of the autonomic preganglionic neurons. Somehow this diminutive structure integrates the diverse information it receives about the body’s status, anticipates some of its needs, and provides a coordinated set of both neural and hormonal outputs. Essential to autonomic control are the connections of the periventricular zone to the brain stem and spinal cord nuclei that contain the preganglionic neurons of the sympathetic and parasympathetic divisions. The nucleus of the solitary tract, located in the medulla and connected with the hypothalamus, is another important center for autonomic control. In fact, some autonomic functions operate well even when the brain stem is disconnected from all structures above it, including the hypothalamus. The solitary nucleus integrates sensory information from the internal organs and coordinates output to the autonomic brain stem nuclei.
Neurotransmitters and the Pharmacology of Autonomic Function
Even people who have never heard the word neurotransmitter know what it means to “get your adrenaline flowing.” (In the United Kingdom, this compound is called adrenaline, while in the United States, it is called epinephrine.) Historically, the autonomic nervous system has probably taught us more than any other part of the body about how neurotransmitters work. Because the ANS is relatively simple compared to the CNS, we understand the ANS much better. In addition, neurons of the peripheral parts of the ANS are outside the blood-brain barrier, so all drugs that enter the bloodstream have direct access to them. The relative simplicity and accessibility of the ANS have led to a deeper understanding of the mechanisms of drugs that influence synaptic transmission.
Preganglionic Neurotransmitters. The primary transmitter of the peripheral autonomic neurons is acetylcholine (ACh), the same transmitter used at skeletal neuromuscular junctions. The preganglionic neurons of both sympathetic and parasympathetic divisions release ACh. The immediate effect is that the ACh binds to nicotinic ACh receptors (nAChR), which are ACh-gated channels, and evokes a fast excitatory postsynaptic potential (EPSP) that usually triggers an action potential in the postganglionic cell. This is very similar to the mechanisms of the skeletal neuromuscular junction, and drugs that block nAChRs in muscle, such as curare, also block autonomic output.
Ganglionic ACh does more than neuromuscular ACh, however. It also activates muscarinic ACh receptors (mAChR), which are metabotropic (G-protein-coupled) receptors that can cause both the opening and the closing of ion channels that lead to very slow EPSPs and IPSPs. These slow mAChR events are usually not evident unless the preganglionic nerve is activated repetitively. In addition to ACh, some preganglionic terminals release a variety of small, neuroactive peptides such as neuropeptide Y (NPY) and vasoactive intestinal polypeptide (VIP). These also interact with G-protein-coupled receptors and can trigger small EPSPs that last for several minutes. The effects of peptides are modulatory; they do not usually bring the postsynaptic neurons to firing threshold, but they make them more responsive to the fast nicotinic effects when they do come along. Since more than one action potential is required to stimulate the release of these modulatory neurotransmitters, the pattern of firing in preganglionic neurons is an important variable in determining the type of postganglionic activity that is evoked.
Postganglionic Neurotransmitters. Postganglionic cells—the autonomic motor neurons that actually trigger glands to secrete, sphincters to contract or relax, and so on—use different neurotransmitters in the sympathetic and parasympathetic divisions of the ANS. Postganglionic parasympathetic neurons release ACh, but those of most parts of the sympathetic division use norepinephrine (NE). Parasympathetic ACh has a very local effect on its targets and acts entirely through mAChRs. In contrast, sympathetic NE often spreads far, even into the blood where it can circulate widely.
The autonomic effects of a variety of drugs that interact with cholinergic and noradrenergic systems can be confidently predicted once you understand some of the autonomic circuitry and chemistry (see Figure 15.9). In general, drugs that promote the actions of norepinephrine or inhibit the muscarinic actions of acetylcholine are sympathomimetic; they cause effects that mimic activation of the sympathetic division of the ANS. For example, atropine, an antagonist of mAChRs, produces signs of sympathetic activation, such as dilation of the pupils. This response occurs because the balance of ANS activity is shifted toward the sympathetic division when parasympathetic actions are blocked. On the other hand, drugs that promote the muscarinic actions of ACh or inhibit the actions of NE are parasympathomimetic; they cause effects that mimic activation of the parasympathetic division of the ANS. For example, propranolol, an antagonist of the β receptor for NE, slows the heart rate and lowers blood pressure. For this reason, propranolol is sometimes used to prevent the physiological consequences of stage fright.
But what about the familiar flow of adrenaline? Adrenaline (epinephrine) is the compound released into the blood from the adrenal medulla when activated by preganglionic sympathetic innervation. Epinephrine is actually made from norepinephrine (called noradrenaline in the United Kingdom), and it has effects on target tissues almost identical to those caused by sympathetic activation. Thus, the adrenal medulla is really nothing more than a modified sympathetic ganglion. You can imagine that as the epinephrine (adrenaline) flows, a coordinated, body-wide set of sympathetic effects kicks in.
Consider what happens when you fall asleep. The internal commands “You are becoming drowsy” and “You are falling asleep” are messages that must be received by broad regions of the brain. Dispensing this information requires neurons with a particularly widespread pattern of axons. The brain has several such collections of neurons, each using a particular neurotransmitter and making widely dispersed, diffuse, almost meandering connections. Rather than carrying detailed sensory information, these cells often perform regulatory functions, modulating vast assemblies of postsynaptic neurons (in structures such as the cerebral cortex, the thalamus, and the spinal cord) so that they become more or less excitable, more or less synchronously active, and so on. Collectively, they are a bit like the volume, treble, and bass controls on a radio, which do not change the lyrics or melody of a song but dramatically regulate the impact of both. In addition, different systems appear to be essential for aspects of motor control, memory, mood, motivation, and metabolic state. Many psychoactive drugs affect these modulatory systems, and the systems figure prominently in current theories about the biological basis of certain psychiatric disorders.
Anatomy and Functions of the Diffuse Modulatory Systems
The diffuse modulatory systems differ in structure and function, yet they have certain principles in common:
- Typically, the core of each system has a small set of neurons (several thousand).
- Neurons of the diffuse systems arise from the central core of the brain, most of them from the brain stem.
- Each neuron can influence many others because each one has an axon that may contact more than 100,000 postsynaptic neurons spread widely across the brain.
- The synapses made by many of these systems release transmitter molecules into the extracellular fluid, so they can diffuse to many neurons rather than be confined to the vicinity of the synaptic cleft.
We’ll focus on the modulatory systems of the brain that use either norepinephrine (NE), serotonin (5-HT), dopamine (DA), or acetylcholine (ACh) as a neurotransmitter. Recall from Chapter 6 that all of these transmitters activate specific metabotropic (G-protein-coupled) receptors, and these receptors mediate most of their effects; for example, the brain has 10–100 times more metabotropic ACh receptors than ionotropic nicotinic ACh receptors.
Because neuroscientists are still working hard to determine the exact functions of these systems in behavior, our explanations here will necessarily be general. It is clear, however, that the functions of the diffuse modulatory systems depend on how electrically active they are, individually and in combination, and on how much neurotransmitter is available for release (Box 15.2).
Americans, it seems, are always trying to lose weight. The low-fat, high-carbohydrate diets (think bagels) that were all the rage in the 1990s were replaced by a low-carb craze (think omelets). Changing your diet can alter caloric intake and the body’s metabolism, and it can also alter how your brain functions.
The influence of diet on the brain is most clear in the case of the diffuse modulatory systems. Consider serotonin. Serotonin is synthesized in two steps from the dietary amino acid tryptophan (see Figure 6.14). In the first step, a hydroxyl group (OH) is added to tryptophan by the enzyme tryptophan hydroxylase. The low affinity of the enzyme for tryptophan makes this step rate-limiting for serotonin synthesis—that is, serotonin can be produced only as fast as this enzyme can hydroxylate tryptophan. And a lot of tryptophan is required to push the synthetic reaction as fast as it can go. However, brain tryptophan levels are well below the level required to saturate the enzyme. Thus, the rate of serotonin synthesis is determined, in part, by the availability of tryptophan in the brain—more tryptophan, more serotonin; less tryptophan, less serotonin.
Brain tryptophan levels are controlled by how much tryptophan is in the blood and by how efficiently it is transported across the blood-brain barrier. Tryptophan in the blood is derived from the proteins we digest in our diet, so a high-protein diet will lead to sharply increased blood levels of tryptophan. Surprisingly, however, there is a decline in brain tryptophan (and serotonin) for several hours after a hearty, high-protein meal. The paradox was resolved by Richard Wurtman and his colleagues at the Massachusetts Institute of Technology who observed that several other amino acids (tyrosine, phenylalanine, leucine, isoleucine, and valine) compete with tryptophan for transport across the blood-brain barrier. These other amino acids are rich in a high-protein diet, and they suppress the entry of the tryptophan into the brain. The situation is reversed with a high-carbohydrate meal that also contains some protein. Insulin, released by the pancreas in response to carbohydrates, decreases the blood levels of the competing amino acids relative to tryptophan. So the tryptophan in the blood is efficiently transported into the brain, and serotonin levels rise.
Increased brain tryptophan correlates with elevated mood, decreased anxiety, and increased sleepiness, likely due to changes in serotonin levels. Inadequate tryptophan may explain the phenomenon of carbohydrate craving that has been reported in humans with seasonal affective disorder—the depression of mood brought on by reduced daylight during winter. It may also explain why clinical trials for treating obesity with extreme carbohydrate deprivation had to be stopped because of complaints of mood disturbances (depression, irritability) and insomnia.
Based on these and other observations, Wurtman and his wife Judith made the intriguing suggestion that our dietary choices may reflect our brain’s need for serotonin. Consistent with this notion, drugs that elevate extracellular serotonin can be effective for weight loss (as well as depression), possibly by reducing the body’s demand for carbohydrates. We will discuss the involvement of serotonin in appetite regulation further in Chapter 16, and in the regulation of mood in Chapter 22.
The Noradrenergic Locus Coeruleus. Besides being a neurotransmitter in the peripheral ANS, NE is also used by neurons of the tiny locus coeruleus in the pons (from the Latin for “blue spot” because of the pigment in its cells). Each human locus coeruleus has about 12,000 neurons. We have two of them, one on each side.
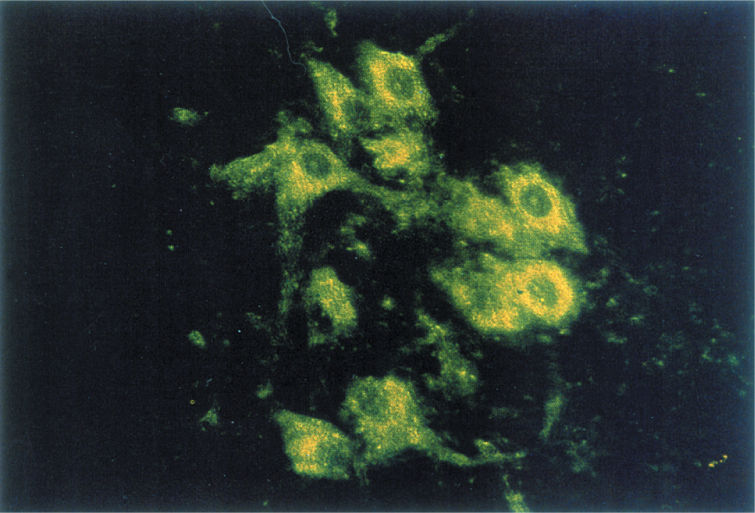
A major breakthrough occurred in the mid-1960s, when Nils-Åke Hillarp and Bengt Falck at the Karolinska Institute in Sweden developed a technique that enabled the catecholaminergic (noradrenergic and dopaminergic) neurons to be visualized selectively in histological sections prepared from the brain (Figure 15.11). This analysis revealed that axons leave the locus coeruleus in several tracts but then fan out to innervate just about every part of the brain: all of the cerebral cortex, the thalamus and the hypothalamus, the olfactory bulb, the cerebellum, the midbrain, and the spinal cord (Figure 15.12). The locus coeruleus makes some of the most diffuse connections in the brain, considering that just one of its neurons can make more than 250,000 synapses, and it can have one axon branch in the cerebral cortex and another in the cerebellar cortex! The organization of this circuitry is so different from what was then known about synaptic connections in the brain that it took many years of research before the mainstream neuroscience community could accept that NE was a neurotransmitter in the brain (Box 15.3).

FIGURE 15.11 Norepinephrine-containing neurons of the locus coeruleus. Reaction of noradrenergic neurons with formaldehyde gas causes them to fluoresce green, enabling anatomical investigation of their widespread projections. (Courtesy of Dr. Kjell Fuxe.)

FIGURE 15.12 The noradrenergic diffuse modulatory system arising from the locus coeruleus. The small cluster of locus coeruleus neurons projects axons that innervate vast areas of the CNS, including the spinal cord, cerebellum, thalamus, and cerebral cortex.
Norepinephrine (NE) was accepted as the neurotransmitter for the peripheral autonomic sympathetic nervous system by the 1930s, but identification of this catecholamine’s status in the brain remained uncharacterized for another three decades. By the late 1950s, central chemical neurotransmission was conceived as an extension to the brain of the then best studied synapse, the neuromuscular junction. Here acetylcholine had satisfied the four identification criteria of a neurotransmitter: localization, mimicry of nerve action, identical pharmacology, and ionic permeability changes. But what other brain chemicals did the brain use for those synapses not mediated by acetylcholine? NE was detected in the brain and was regionally distributed (rich in hypothalamus, low in cortex), which was incompatible with it being simply the sympathetic innervation of the brain’s blood vessels, but what did it do?
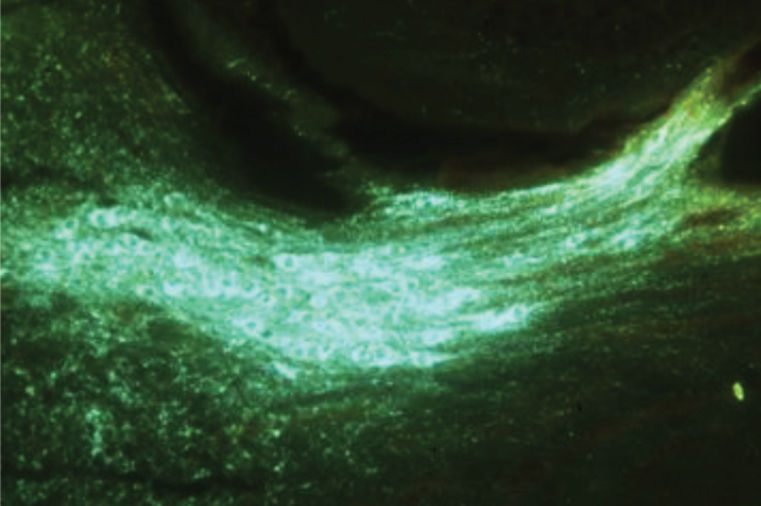
When I went to the National Institutes of Health (NIH) in 1962 to avoid the “Doctor’s Draft” into the Army, I spent 2 years assessing how neurons in the hypothalamus, olfactory bulb, and striatum respond to NE applied by microionophoresis. The results appeared random: A third fired faster, a third fired slower, and the remaining third were unresponsive. What was missing was knowledge of which neurons, if any, were actually innervated by NE fibers. This critical information was provided when the Swedish scientists Nils-Åke Hillarp and Bengt Falck developed a histochemical method, called formaldehyde-induced fluorescence, which caused monoamines (NE, dopamine, and serotonin) to fluoresce when illuminated with the appropriate wavelength of light. But in the humid climate of Washington D.C., I could not replicate their findings. I therefore went to Yale to try different approaches using electron microscopy and autoradiography to see which nerve terminals could concentrate radioactive NE, as Julius Axelrod had done for the sympathetic innervation of the pineal body.
When I returned to NIH in 1968, I had learned enough to suspect that cerebellar Purkinje neurons were targets of synapses utilizing NE as a neurotransmitter. This was also the best understood region of the brain in terms of cellular circuitry. Together with Barry Hoffer, who had studied cerebellar development, and George Siggins, who was expert in the sympathetic innervation of peripheral blood vessels, we set about to test how Purkinje neurons respond to NE. We found that they responded consistently by slowing their spontaneous activity. This effect was blocked by norepinephrine beta receptor antagonists and was prolonged by NE reuptake inhibitors, and both effects were lost when the NE neurons were destroyed with the toxin 6-hydroxydopamine.
While visiting the Karolinska Institute in 1971 (the year Axelrod was awarded the Nobel Prize), I learned from Lars Olson and Kjell Fuxe that the locus coeruleus in the pons provided the NE innervation of the cerebellum as well as the entire forebrain (Figure A). When Siggins, Hoffer, and I electrically stimulated the locus coeruleus, Purkinje cell firing slowed, thus mimicking the effects of NE by microionophoresis. The effect of locus coeruleus stimulation was lost when NE was depleted using inhibitors of tyrosine hydroxylase, or eradicated with 6-hydroxydopamine. At last, we were convinced that NE satisfied the neurotransmitter identification criteria. But clearly, the CNS actions of NE differed dramatically from those of “classical” fast central transmitter systems. Instead of being strictly excitatory or inhibitory, NE seemed to act to enhance the effects of other afferent projections to the same postsynaptic targets. Menahem Segal, working with me at the NIH, reached a similar conclusion for the actions of NE in the hippocampus.

Figure A Green fluorescent NE neurons in a sagittal section of the rat locus coeruleus. (Source: Courtesy of Dr. Floyd Bloom, The Scripps Research Institute.)
After moving to the Salk Institute, I worked with Steve Foote and Gary Aston-Jones to record the firing patterns of the locus coeruleus neurons in awake behaving rats and squirrel monkeys. These experiments revealed that the locus coeruleus neurons have brief phasic responses to novel sensory signals of all modalities, progressively slowing with loss of attention and becoming silent during rapid eye movement sleep. The phasic and tonic discharge modes correlate with the chemical thresholds for alpha (highly sensitive) and beta (less sensitive) adrenergic receptors.
Subsequently, using immunohistochemistry with antibodies to the enzyme dopamine-beta-hydroxylase, found only in NE-containing neurons, Steve Foote, John Morrison, David Lewis, and I generated detailed NE circuit maps in the nonhuman primate brain. In contrast to the diffuse rodent cortical innervations, their data showed differences in the amount of innervation in architectonically defined areas of the cerebral cortex, particularly in the cingulate and orbitofrontal cortex. This map suggested that the locus coeruleus-NE afferents have a greater influence on spatial and visuomotor detection than on detailed sensory feature detection. My interests in the central catecholamine systems and brain disease continue today and have been intensified by the computational and theoretical concepts now being developed from studies of the roles of these systems in awake behaving primates, including normal cognitive declines with aging.
Locus coeruleus cells seem to be involved in the regulation of attention, arousal, and sleep–wake cycles as well as learning and memory, anxiety and pain, mood, and brain metabolism. This makes it sound as if the locus coeruleus may run the whole show. But the key word is “involved,” which can mean almost anything. For example, our heart, liver, lungs, and kidneys are also involved in every brain function, for without them, the brain cannot survive. Because of its widespread connections, the locus coeruleus can influence virtually all parts of the brain. But to understand its actual functions, we start by determining what activates its neurons. Recordings from awake, behaving rats and monkeys show that locus coeruleus neurons are most strongly activated by new, unexpected, nonpainful sensory stimuli in the animal’s environment. They are least active when the animals are not vigilant, just sitting around quietly, digesting a meal. The locus coeruleus may participate in a general arousal of the brain during interesting events in the outside world. Because NE can make neurons of the cerebral cortex more responsive to salient sensory stimuli, the locus coeruleus may function generally to increase brain responsiveness, speeding information processing by the point-to-point sensory and motor systems and making them more efficient.
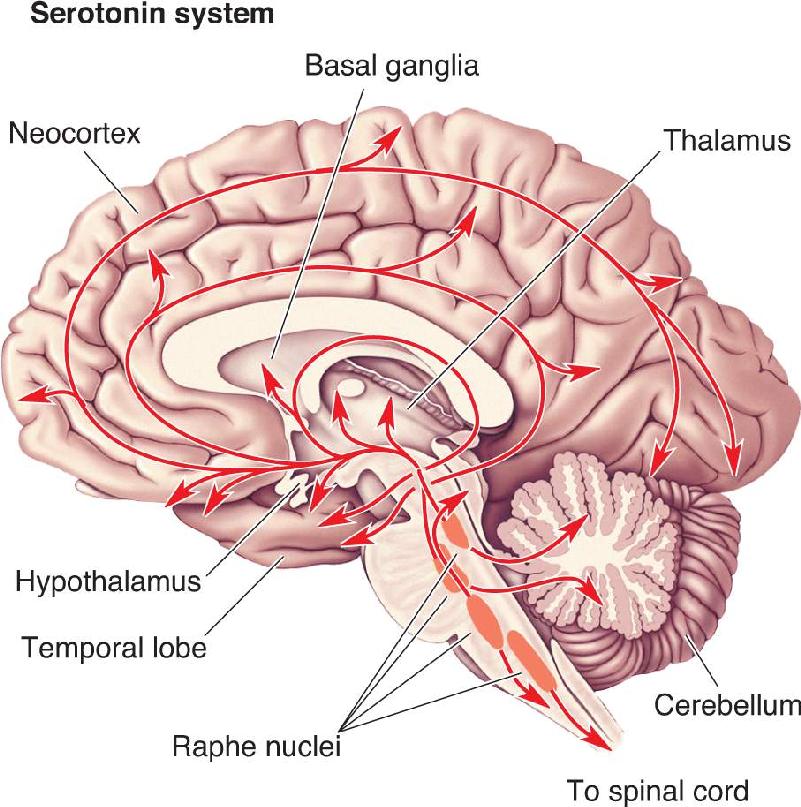
The Serotonergic Raphe Nuclei. Serotonin-containing neurons are mostly clustered within the nine raphe nuclei. Raphe means “ridge” or “seam” in Greek, and, indeed, the raphe nuclei lie to either side of the midline of the brain stem. Each nucleus projects to different regions of the CNS (Figure 15.13). Those more caudal, in the medulla, innervate the spinal cord, where they modulate pain-related sensory signals (see Chapter 12). Those more rostral, in the pons and midbrain, innervate most of the brain in much the same diffuse way as do the locus coeruleus neurons.

FIGURE 15.13 The serotonergic diffuse modulatory systems arising from the raphe nuclei. The raphe nuclei are clustered along the midline of the brain stem and project extensively to all levels of the CNS. Description
Similar to neurons of the locus coeruleus, raphe nuclei cells fire most rapidly during wakefulness, when an animal is aroused and active. Raphe neurons are the most quiet during sleep. The locus coeruleus and the raphe nuclei are part of a venerable concept called the ascending reticular activating system, which implicates the reticular “core” of the brain stem in processes that arouse and awaken the forebrain. This simple idea has been refined and redefined in countless ways since it was introduced in the 1950s, but its basic sense remains. Raphe neurons seem to be intimately involved in the control of sleep–wake cycles, as well as the different stages of sleep. It is important to note that several other transmitter systems are involved in a coordinated way as well. We will discuss the involvement of the diffuse modulatory systems in sleep and wakefulness in Chapter 19.
Serotonergic raphe neurons have also been implicated in the control of mood and certain types of emotional behavior. We will return to serotonin and mood when we discuss clinical depression in Chapter 22.
The Dopaminergic Substantia Nigra and Ventral Tegmental Area. For many years, neuroscientists thought that dopamine existed in the brain only as a metabolic precursor for norepinephrine. However, research conducted in the 1960s by Arvid Carlsson of the University of Gothenburg in Sweden proved that dopamine was indeed a crucial CNS neurotransmitter. This discovery was honored with the 2000 Nobel Prize in Medicine.
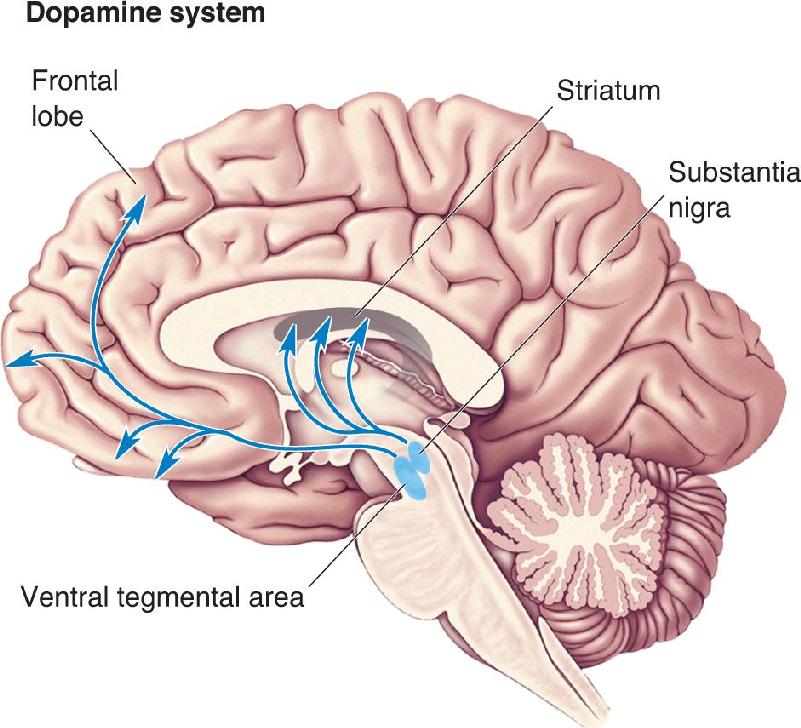
Although there are dopamine-containing neurons scattered throughout the CNS, including some in the retina, the olfactory bulb, and the periventricular hypothalamus, two closely related groups of dopaminergic cells have the characteristics of the diffuse modulatory systems (Figure 15.14). One of these arises in the substantia nigra in the midbrain. Recall from Chapter 14 that these cells project axons to the striatum (the caudate nucleus and the putamen), where they somehow facilitate the initiation of voluntary movements. Degeneration of the dopamine-containing cells in the substantia nigra is all that is necessary to produce the progressive, dreadful motor disorders of Parkinson’s disease. Although we do not entirely understand the function of DA in motor control, in general it facilitates the initiation of motor responses by environmental stimuli.

FIGURE 15.14 The dopaminergic diffuse modulatory systems arising from the substantia nigra and the ventral tegmental area. The substantia nigra and ventral tegmental area lie close together in the midbrain. They project to the striatum (caudate nucleus and putamen) and limbic and frontal cortical regions, respectively. Description
The midbrain is also the origin of the other dopaminergic modulatory system, a group of cells that lie very close to the substantia nigra, in the ventral tegmental area. Axons from these neurons innervate a circumscribed region of the telencephalon that includes the frontal cortex and parts of the limbic system. (The limbic system will be discussed in Chapter 18.) This dopaminergic projection from the midbrain is sometimes called the mesocorticolimbic dopamine system. A number of different functions have been ascribed to this complicated projection. For example, evidence indicates that it is involved in a “reward” system that somehow assigns value to, or reinforces, certain behaviors that are adaptive. We will see in Chapter 16 that if rats (or humans) are given a chance to do so, they will work to electrically stimulate this pathway. In addition, this projection has been implicated in psychiatric disorders, as we will discuss in Chapter 22.
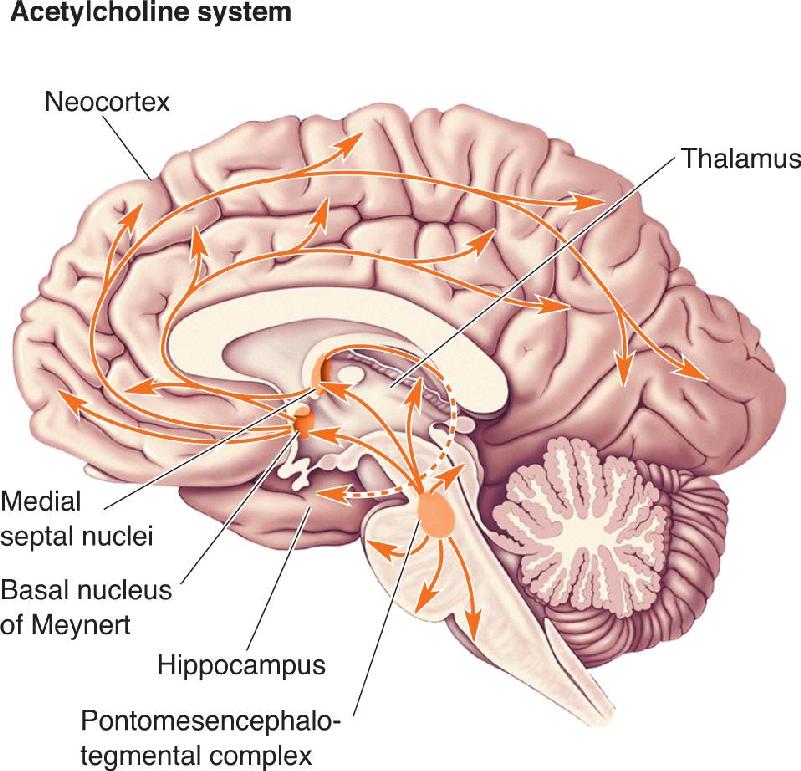
The Cholinergic Basal Forebrain and Brain Stem Complexes. Acetylcholine is the familiar transmitter at the neuromuscular junction, at synapses in autonomic ganglia, and at postganglionic parasympathetic synapses. Cholinergic interneurons also exist within the brain—in the striatum and the cortex, for example. In addition, there are two major diffuse modulatory cholinergic systems in the brain, one of which is called the basal forebrain complex. It is a “complex” because the cholinergic neurons lie scattered among several related nuclei at the core of the telencephalon, medial and ventral to the basal ganglia. The best known of these are the medial septal nuclei, which provide the cholinergic innervation of the hippocampus, and the basal nucleus of Meynert, which provides most of the cholinergic innervation of the neocortex.
The function of the cells in the basal forebrain complex remains mostly unknown. But interest in this region has been fueled by the discovery that these are among the first cells to die during the course of Alzheimer’s disease, which is characterized by a progressive and profound loss of cognitive functions. (However, there is widespread neuronal death in Alzheimer’s disease, and no specific link between the disease and cholinergic neurons has been established.) Like the noradrenergic and serotonergic systems, the cholinergic system has been implicated in regulating general brain excitability during arousal and sleep–wake cycles. The basal forebrain complex may also play a special role in learning and memory formation.
The second diffuse cholinergic system is called the pontomesencephalotegmental complex. These are ACh-utilizing cells in the pons and midbrain tegmentum. This system acts mainly on the dorsal thalamus, where, together with the noradrenergic and serotonergic systems, it regulates the excitability of the sensory relay nuclei. These cells also project up to the telencephalon, providing a cholinergic link between the brain stem and basal forebrain complexes. Figure 15.15 shows the cholinergic systems.

FIGURE 15.15 The cholinergic diffuse modulatory systems arising from the basal forebrain and brain stem. The medial septal nuclei and basal nucleus of Meynert project widely upon the cerebral cortex, including the hippocampus. The pontomesencephalotegmental complex projects to the thalamus and parts of the forebrain. Description
Psychoactive drugs, compounds with “mind-altering” effects, all act on the central nervous system, and most do so by interfering with chemical synaptic transmission. Many abused drugs act directly on the modulatory systems, particularly the noradrenergic, dopaminergic, and serotonergic systems.
Hallucinogens. The use of hallucinogens, drugs that produce hallucinations, goes back thousands of years. Hallucinogenic compounds are contained in a number of plants consumed as part of religious ritual, for example, the Psilocybe mushroom by the Maya and the peyote cactus by the Aztec. The modern era of hallucinogenic drug use was unwittingly ushered in at the laboratory of Swiss chemist Albert Hofmann. In 1938, Hofmann chemically synthesized a new compound, lysergic acid diethylamide (LSD). For 5 years, the LSD sat on the shelf. Then one day in 1943, Hofmann accidentally ingested some of the powder. His report on the effects attracted the immediate interest of the medical community. Psychiatrists began to use LSD in attempts to unlock the subconscious of mentally disturbed patients. Later the drug was discovered by intellectuals, artists, students, and the U.S. Defense Department, who investigated its “mind-expanding” effects. (A chief advocate of LSD use was former Harvard psychologist Timothy Leary.) In the 1960s, LSD made its way to the street and was widely abused. It is illegal to possess LSD today.
LSD is extremely potent. A dose of only 25 μg is sufficient to produce a full-blown hallucinogenic effect (compared to a normal dose of aspirin at 650 mg, which is 25,000 times larger). Among the reported behavioral effects of LSD are a dreamlike state with heightened awareness of sensory stimuli, often with a mixing of perceptions such that sounds can evoke images, images can evoke smells, and so on.
The chemical structure of LSD (and the active ingredients of Psilocybe mushrooms and peyote) is very close to that of serotonin, suggesting that it acts on the serotonergic system. Indeed, LSD is a potent agonist at the serotonin receptors on the presynaptic terminals of neurons in the raphe nuclei. Activation of these receptors markedly inhibits the firing of raphe neurons. Thus, one known CNS effect of LSD is a reduction in the outflow of the brain’s serotonergic diffuse modulatory system. It is interesting to note in this regard that decreased activity of the raphe nuclei is also characteristic of dream-sleep (see Chapter 19).
Can we conclude that LSD produces hallucinations by silencing the brain’s serotonin systems? If only drug effects on the brain were that simple. Unfortunately, there are problems with this hypothesis. For one, silencing neurons in the raphe nuclei by other means—by destroying them, for example—does not mimic the effects of LSD in experimental animals. Furthermore, animals still respond as expected to LSD after their raphe nuclei have been destroyed.
In recent years, researchers have focused on direct LSD actions at serotonin receptors in the cerebral cortex. Current research suggests that LSD causes hallucinations by superseding the naturally modulated release of serotonin in cortical areas where perceptions normally are formed and interpreted.
Stimulants. In contrast to the uncertainties about hallucinogens and serotonin, it is clear that the powerful CNS stimulants cocaine and amphetamine both exert their effects at synapses made by dopaminergic and noradrenergic systems. Both drugs give users a feeling of increased alertness and self-confidence, a sense of exhilaration and euphoria, and a decreased appetite. Both are also sympathomimetic—they cause peripheral effects that mimic activation of the sympathetic division of the ANS: increased heart rate and blood pressure, dilation of the pupils, and so on.
Cocaine is extracted from the leaves of the coca plant and has been used by Andean indigenous peoples for hundreds of years. In the mid-nineteenth century, cocaine turned up in Europe and North America as the magic ingredient in a wide range of concoctions touted as having medicinal value. (An example is Coca-Cola, originally marketed in 1886 as a therapeutic agent, which contained both cocaine and caffeine.) Cocaine use fell out of favor early in the twentieth century, only to reemerge in the late 1960s as a popular recreational drug. Ironically, one of the main reasons for the rise in cocaine use during this period was the tightening of regulations against amphetamines. First chemically synthesized in 1887, amphetamines did not come into wide use until World War II, when they were taken by soldiers (particularly aviators) to sustain them in combat. Following the war, amphetamines became available as nonprescription diet aids, as nasal decongestants, and as “pep pills.” Regulations were finally tightened after recognition that amphetamines are, like cocaine, highly addictive and dangerous in large doses.
The neurotransmitters dopamine and norepinephrine are catecholamines, named for their chemical structure (see Chapter 6). The actions of catecholamines released into the synaptic cleft are normally terminated by specific uptake mechanisms. Cocaine and amphetamine both block this catecholamine uptake (Figure 15.16). However, recent work suggests that cocaine targets DA reuptake more selectively; amphetamine blocks NE and DA reuptake and stimulates the release of DA. Thus, these drugs can prolong and intensify the effects of released DA or NE. Is this the means by which cocaine and amphetamine cause their stimulant effects? There is good reason for thinking so. For example, experimental depletion of brain catecholamines by using synthesis inhibitors (such as α-methyltyrosine) will abolish the stimulant effects of both cocaine and amphetamine.

FIGURE 15.16 Stimulant drug action on the catecholamine axon terminal. On the left is a noradrenergic terminal, and on the right is a dopaminergic terminal. Both neurotransmitters are catecholamines synthesized from the dietary amino acid tyrosine. Dopa (3, 4-dihydroxypheynylalanine) is an intermediate in the synthesis of both. The actions of NE and DA are usually terminated by uptake back into the axon terminal. Amphetamine and cocaine block this uptake, thereby allowing NE and DA to remain in the synaptic cleft longer. Description
Besides having a similar stimulant effect, cocaine and amphetamine share another, more insidious behavioral action: psychological dependence, or addiction. Users will develop powerful cravings for prolonging and continuing drug-induced pleasurable feelings. These effects are believed to result specifically from the enhanced transmission in the mesocorticolimbic dopamine system during drug use. Remember, this system may normally function to reinforce adaptive behaviors. By short-circuiting the system, these drugs instead reinforce drug-seeking behavior. Indeed, just as rats will work to electrically stimulate the mesocorticolimbic projection, they will also work to receive an injection of cocaine. We’ll discuss the involvement of dopamine pathways in motivation and addiction further in Chapter 16.
In this chapter, we have examined three components of the nervous system that are characterized by the great reach of their influences. The secretory hypothalamus and autonomic nervous system communicate with cells all over the body, and the diffuse modulatory systems communicate with neurons in many different parts of the brain. They are also characterized by the duration of their direct effects, which can range from minutes to hours. Finally, they are characterized by their chemical neurotransmitters. In many instances, the transmitter defines the system. For example, in the peripheral nervous system, we can use the words “noradrenergic” and “sympathetic” interchangeably. The same thing goes for “raphe” and “serotonin” in the forebrain, and “substantia nigra” and “dopamine” in the basal ganglia. These chemical idiosyncrasies have allowed interpretations of drug effects on behavior that are not possible with most other neural systems. Thus, we have a good idea where in the brain amphetamine and cocaine exert their stimulant effects, and where outside the CNS, they act to raise blood pressure and heart rate.
At a detailed level, each of the systems discussed in this chapter performs different functions. But at a general level, they all maintain brain homeostasis: They regulate different processes within a certain physiological range. For example, the ANS regulates blood pressure within a range that is appropriate. Blood pressure variations optimize an animal’s performance under different conditions. In a similar way, the noradrenergic locus coeruleus and serotonergic raphe nuclei regulate levels of consciousness and mood. These levels also vary within a range that is adaptive to the organism. In the next several chapters, we will encounter these systems again in the context of specific functions.
1. Battlefield trauma victims who have lost large volumes of blood often express a craving to drink water. Why?
2. You’ve stayed up all night trying to meet a term paper deadline. You now are typing frantically, keeping one eye on the paper and the other on the clock. How has the periventricular zone of the hypothalamus orchestrated your body’s physiological response to this stressful situation? Describe in detail.
3. An “Addisonian crisis” describes a constellation of symptoms that include extreme weakness, mental confusion, drowsiness, low blood pressure, and abdominal pain. What causes these symptoms and what can be done to treat them?
4. Why is the adrenal medulla often referred to as a modified sympathetic ganglion? Why isn’t the adrenal cortex included in this description?
5. A number of famous athletes and entertainers have accidentally killed themselves by taking large quantities of cocaine. Usually the cause of death is heart failure. How would you explain the peripheral actions of cocaine?
6. How do the diffuse modulatory and point-to-point synaptic communication systems in the brain differ? List four ways.
7. Under what behavioral conditions are the noradrenergic neurons of the locus coeruleus active? The noradrenergic neurons of the ANS?
Bloom FE. 2010. The catecholamine neuron: historical and future perspectives. Progress in Neurobiology 90:75–81.
Carlsson A. 2001. A paradigm shift in brain research. Science 294:1021–1024.
McEwen BS. 2002. Sex, stress and the hippocampus: allostasis, allostatic load and the aging process. Neurobiology of Aging 23(5):921–939.
Meyer JS, Quenzer LF. 2004. Psychopharmacology: Drugs, the Brain, and Behavior. Sunderland, MA: Sinauer.
Wurtman RJ, Wurtman JJ. 1989. Carbohydrates and depression. Scientific American 260(1): 68–75.
Additional figures