29 Diagnosing Infectious Diseases
II Isolating and Characterizing Infectious Microorganisms
III Immunological and Molecular Tools for Disease Diagnosis
Shedding New Light on Diagnosing Tuberculosis
Few pathogens have caused more human deaths than Mycobacterium tuberculosis (photo), the causative agent of tuberculosis (TB). Due to the slow growth of M. tuberculosis and the sluggish progression of symptoms associated with TB, it can be difficult to rapidly and reliably detect active disease using traditional diagnostic tools. Further complicating the matter is that the prevalence of TB is high in less developed countries where adequate medical facilities or diagnostic supplies are often lacking. These factors can cause delayed diagnosis of TB, which compromises both patient care and public health efforts to control the disease.

For these reasons, a quick and reliable point-of-care diagnostic test for TB is sorely needed, and one may soon be on the way. Trehalose, a sugar that has been increasingly used as a food additive in recent years, is a precursor building block for the structurally unusual cell wall of M. tuberculosis. With this in mind, researchers have recently targeted trehalose as a chemical marker to reveal the presence of M. tuberculosis in clinical specimens, such as in the sputum samples of patients suspected of having TB.
To use trehalose incorporation as a diagnostic assay, the sugar molecule had to be chemically modified to make it easily detectable. The indicator dye 4-N,N-dimethylamino-1, 8-naphthalimide (DMN) was chosen for this purpose because it fluoresces brightly in a hydrophobic environment. By conjugating DMN to trehalose (creating DMN-Tre) and subsequently allowing living M. tuberculosis cells to incorporate the metabolized DMN-Tre into their waxy (and thus hydrophobic) cell wall, the researchers were, within minutes, able to easily and specifically visualize cells of the glowing pathogen in sputum samples. In addition, because only healthy, growing cells incorporate DMN-Tre and fluoresce, this method may also provide a quick way to determine antibiotic susceptibility for individualized treatment plans.
Source: Kamariza, M., et al. 2018. Rapid detection of Mycobacterium tuberculosis in sputum with a solvatochromic trehalose probe. Sci. Transl. Med. 10: eaam6310. doi:10.1126/scitranslmed.aam6310.
I Microbiology and the Healthcare Environment
Considering the prevalence of multidrug-resistant pathogens and healthcare-associated infections, the importance of safety protocols and personal protective equipment in the clinical microbiology laboratory cannot be overstated.
Clinical microbiology is a subdiscipline of microbiology whose focus is diagnosing infectious diseases by identifying pathogenic microbes and advising medical providers on treatment. Clinical laboratories must identify pathogens safely, efficiently, and reliably. The clinical microbiologist examines patient samples using direct observation, culture, immunological assays, and molecular tools to identify particular pathogens and rule out infection by others. Rapid and accurate identification of pathogens is critical for developing successful treatment strategies and maintaining disease control.
29.1 The Clinical Microbiology Laboratory
Clinical laboratories handle dangerous materials, and thus laboratory workers must adhere to strict safety protocols to prevent the spread of infectious agents. Standard laboratory practices for handling clinical samples have been established to minimize the risk of accidental laboratory infections. One only has to be reminded of the 2014 Ebola hemorrhagic fever outbreak in West Africa (Section 31.12) to appreciate how treating infected persons without paying rigorous attention to every safety detail can endanger the lives of medical personnel.
Laboratory Safety
The clinical laboratory has potential biohazards for all personnel and is especially dangerous for untrained personnel or those who do not employ the necessary precautions. All laboratories that handle human or primate tissue must have an occupational exposure control plan for handling bloodborne pathogens. This plan is specifically designed to protect workers from infection by hepatitis B virus (HBV, the cause of infectious hepatitis, Section 31.11) and human immunodeficiency virus (HIV, the cause of acquired immunodeficiency syndrome [AIDS], Section 31.15). The occupational exposure plan limits infection by all pathogens and typically includes the use of appropriate personal protective equipment (PPE), which includes a lab coat, gloves, eye protection, and face mask (Figure 29.1).
Figure 29.1 Standard apparel for clinical laboratory safety.

This technician is wearing proper personal protective equipment (PPE) for a clinical laboratory, including gloves, eye protection, lab coat, and face mask.
Mastering Microbiology
Art Activity: Table 29.1 Microbiology laboratory safety standards
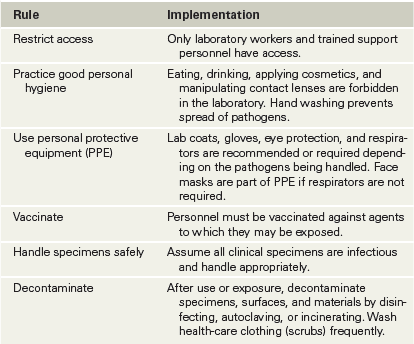
Proper training and enforcement of established safety procedures can prevent most accidental infections, which usually do not result from identifiable exposures like culture spills but instead from routine handling of patient specimens. Infectious aerosols generated during microbiological procedures are the most common causes of laboratory infections. Clinical laboratories follow the safety rules outlined in Table 29.1 to minimize laboratory infections. These general standards apply to all laboratories that handle potentially infectious agents and are the basis for all aspects of healthcare infection control. However, as discussed next, laboratories that handle particularly dangerous or transmissible agents adhere to additional rules and procedures to ensure a safe work environment.
Table 29.1 Microbiology laboratory safety standards

Biological Containment and Biosafety Levels
The level of containment used to prevent accidental infections or accidental environmental contamination (escape) in clinical, research, and teaching laboratories must be proportional to the biohazard potential of the organisms handled in the laboratory. Laboratories are classified according to their containment capabilities from least to greatest by their biosafety level (BSL), designated as BSL-1, BSL-2, BSL-3, or BSL-4 (Figure 29.2). Personnel in laboratories working at all biosafety levels must follow standard laboratory practices that ensure basic cleanliness and limit contamination (Table 29.1). The precautions, equipment, and operational costs increase with each biosafety level, but the rationale in each case is the same: Keep any potentially infectious agents confined to the laboratory.
Figure 29.2 Conducting research in a BSL-4 (biosafety level 4) laboratory.


BSL-4 is the highest level of biological control, affording maximum worker protection and pathogen containment. The researcher has a whole-body sealed suit with an outside air supply and ventilation system. Air locks control all access to the laboratory. All material leaving the laboratory is autoclaved or chemically decontaminated.
Most colleges and universities have BSL-1 and BSL-2 laboratories for teaching and research. Standard clinical laboratories operate at BSL-2. The specialized physical requirements for BSL-3 facilities limit them to major clinical centers and research settings. Because BSL-4 facilities must ensure total isolation and physical containment of pathogens, only about fifty BSL-4 laboratories are operational worldwide. Most BSL-4 laboratories are associated with government facilities, such as the Centers for Disease Control and Prevention (CDC; Atlanta, Georgia, USA) and the U.S. Army Medical Research Institute of Infectious Diseases (USAMRIID; Fort Detrick, Maryland, USA).
Check Your Understanding
The use of personal protective equipment (PPE) is required for clinical laboratory technicians. What protective apparel does PPE include?
Identify and discuss the standard safety procedures adopted by microbiology laboratories. Under what biosafety level do most clinical laboratories operate? With what type of facility are most BSL-4 laboratories associated?
29.2 Healthcare-Associated Infections
The universal safety measures described in the previous section are implemented to contain infectious agents and prevent their transmission in laboratory settings. But despite the routine use of gloves and clean clinical clothing (“hospital scrubs”) in healthcare facilities, the accidental transfer of pathogens to patients in these environments is a common occurrence.
Mechanisms of Transfer of Healthcare-Associated Infections
A healthcare-associated infection (HAI), also called a nosocomial infection (from the Latin nosocomium, meaning hospital), is an infection acquired by a patient during a stay at a healthcare facility (clinic, hospital, rehabilitation facility, etc.). HAIs cause significant morbidity (incidence of disease in a population) and mortality (incidence of death in a population). An estimated 10% of patients admitted to healthcare facilities in the United States acquire HAIs, and up to 2 million HAIs occur annually, leading directly or indirectly to about 75,000 deaths. Some of the common risk factors for acquiring infectious diseases in healthcare settings are summarized in Table 29.2.
Table 29.2 Risk factors for hospital-acquired infections (HAIs)

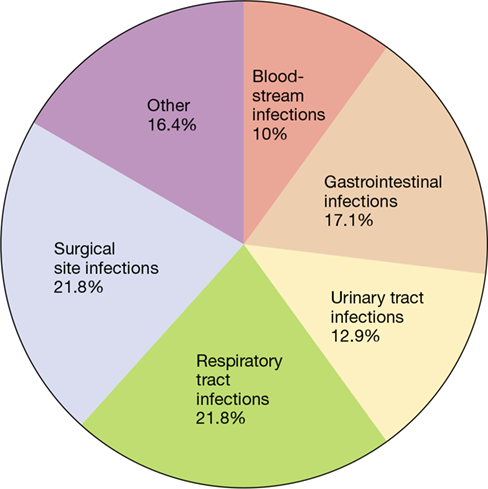
Some HAIs are acquired from patients with communicable diseases, but others are caused by pathogens that are selected for and maintained within the hospital environment, spread by cross-infection from patient to patient or from healthcare personnel. Healthcare-associated pathogens are often present as normal microbiota in either patients or healthcare staff. Therefore, healthcare facilities are high-risk environments for the spread of infections because these facilities concentrate individuals who have infectious disease or are at risk for acquiring infectious disease because of underlying health conditions. Such conditions often lead to a compromised immune system and increased susceptibility to pathogens. The frequency of HAIs at different sites of the body is shown in Figure 29.3.
Figure 29.3 Frequency of healthcare-associated infections (HAIs) in different sites of the body.

Up to 2 million HAIs occur annually in the United States. Data are from the Centers for Disease Control and Prevention.
Mastering Microbiology
Art Activity: Figure 29.3 Frequency of healthcare-associated infections (HAIs) in different sites of the body
Common Causative Agents of HAIs
Most HAIs are caused by a relatively short list of pathogens (Table 29.3), but many other infectious agents can cause HAIs. Staphylococcus aureus is one of the most important and widespread HAI pathogens (Section 31.9). It is the most common cause of pneumonia, the third most common cause of blood infections, and is particularly problematic in nurseries. Many hospital strains of S. aureus are unusually virulent and are resistant to common antibiotics, making treatment especially difficult (see Explore the Microbial World, “MRSA—A Formidable Clinical Challenge”). The staphylococci are the most common cause of bloodborne HAIs and are also prevalent in pus-forming wound infections.
Table 29.3 Common healthcare-associated pathogens

Staphylococcus and Enterococcus, as well as Escherichia coli, Klebsiella pneumoniae, and various other Enterobacteriaceae, all have the potential to cause HAIs, but they are also members of the normal microbiota of most individuals, making it essentially impossible to eliminate these potential pathogens from healthcare settings. In addition, these organisms can acquire multidrug resistance by horizontal gene flow (Chapter 9). Pathogens that are not part of the normal microbiota, such as species of Acinetobacter and Mycobacterium, can be eliminated from the healthcare environment. These pathogens are carried into the healthcare facilities by infected individuals or, in the case of some mycobacteria, as airborne contaminants.
Prevention of HAIs requires cooperation between the healthcare facility infection-control team and the rest of the facility staff, including direct healthcare workers and supporting staff, such as housekeeping. Infection control starts with management of incoming patients at the point of entry to the healthcare facility; incoming patients should be assessed for possible infections and isolated as necessary to prevent spread of infections to staff and other patients. In addition, periodic testing of healthcare personnel for key pathogens, such as methicillin-resistant Staphylococcus aureus (MRSA), can identify healthy carriers. From this point, the healthcare facility staff employs standard procedures that limit infection, applying the same general precautions outlined for laboratory technicians in Table 29.1.
Check Your Understanding
Why are patients in healthcare facilities especially susceptible to pathogens?
II: Isolating and Characterizing Infectious Microorganisms
II: Isolating and Characterizing Infectious Microorganisms
II Isolating and Characterizing Infectious Microorganisms
Although the emphasis on molecular diagnostic tools is growing in clinical laboratories, traditional specimen collection and pathogen cultivation techniques are universally used and provide accurate disease diagnosis in a timely manner.
The growth and observation of pathogens from patient specimens are important strategies for identification of the causative agent of an infectious disease. Identification leads to antimicrobial drug susceptibility testing and development of a specific treatment plan. We begin by looking at methods for collecting, culturing, and identifying pathogens, followed by methods used to determine drug susceptibility.
29.3 Workflow in the Clinical Laboratory
Collecting specimens from infectious patients and subsequently culturing pathogens using a variety of growth media is a necessary and routine practice in clinical medicine. Combined with microscopic observation, these methods allow for direct detection and identification of causative agents of disease.
Collecting Specimens and Detecting and Culturing Pathogens
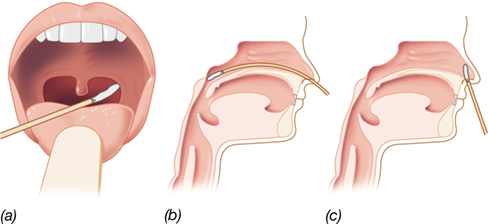
Proper clinical diagnosis of infectious diseases requires that pathogens be identified from tissue or fluid samples using a variety of microbiological, immunological, and molecular biological techniques (Figure 29.4). Patient specimens must be collected aseptically from the site of the infection, and the sample size must be large enough to ensure an inoculum sufficient for growth. In addition, the requirements for organism survival, such as oxic versus anoxic conditions, must be maintained at all times, and the sample should be processed quickly to avoid degradation. Sterile swabs are often used to obtain samples from infected areas, including wounds, nares, or throat (Figure 29.5), and the swab is then used to inoculate a suitable growth medium.
Figure 29.4 Laboratory identification of microbial pathogens.

The flowchart shows alternative paths for identifying pathogens or pathogen exposure in the clinical laboratory.
Figure 29.5 Specimens from the upper respiratory tract.

(a) Throat swab. (b) Nasopharyngeal swab passed through the nose. (c) Swabbing the inside of the nose.
Mastering Microbiology
Art Activity: Figure 29.4 Laboratory identification of microbial pathogens
Many pathogens can be detected by direct means using one or more of several diagnostic tests. For example, the microscopic observation of gram-negative diplococci, especially inside neutrophil inclusions, in a urethral exudate sample is diagnostic for infection with Neisseria gonorrhoeae (**Figure 29.6*a***), the causative agent of the sexually transmitted disease gonorrhea (Section 31.13). However, the reliability of any diagnostic test depends on both the specificity and the sensitivity of the test. Specificity is the ability of the test to recognize a single pathogen. High specificity reduces the likelihood of a false-positive result. Sensitivity defines the smallest quantity of a pathogen or a pathogen product that can be detected. High sensitivity minimizes the likelihood of a false-negative reaction. For the detection of N. gonorrhoeae, the specificity of Gram-stained smears of urogenital exudates is high for both men and women (≥95%), so false-positive tests for gonorrhea are rare. By contrast, the sensitivity of Gram-stained smears of urogenital exudates for the detection of N. gonorrhoeae is about 80% greater for men than for women. Thus, in suspected cases of gonorrhea in females, false-negative Gram stains are relatively common. Females must therefore be examined by more sensitive methods, including culture techniques (Figure 29.6b), to establish or confirm a diagnosis of gonorrhea.
Figure 29.6 Identification of *Neisseria gonorrhoeae*, the cause of gonorrhea.

(a) Cells of gram-negative N. gonorrhoeae within human polymorphonuclear leukocytes (neutrophils) from a urethral exudate. (b) Colonies of N. gonorrhoeae growing on a filter placed on Thayer–Martin agar. Oxidase reagent, which turns colonies dark purple if they contain cytochrome c, has been added to the filter. The dark color of the colonies shows that N. gonorrhoeae is oxidase-positive.
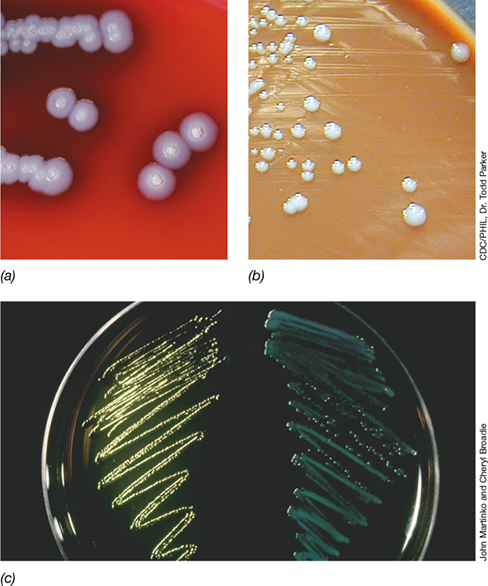
Specific pathogens can be selectively grown, isolated, and identified from patient specimens using specialized growth media and incubation conditions to establish an enrichment culture (Sections 19.1 and 19.2). For primary enrichment, clinical samples are inoculated on general-purpose media, such as blood agar (**Figure 29.7*a***) and chocolate agar (so called because it contains heat-lysed blood, making it brown in color; Figure 29.7b), which support the growth of a variety of microorganisms. To aid in the isolation and identification of specific pathogens, medical technologists use various selective and differential growth media. Selective media are specialized culture media that contain inhibitory agents for the purpose of allowing some organisms to grow but not others. Differential media allow identification of organisms based on the appearance of the culture after growth. For example, eosin–methylene blue (EMB) agar is a selective medium because the methylene blue it contains inhibits the growth of gram-positive bacteria. EMB agar is also a differential medium because it distinguishes gram-negative bacteria that can ferment lactose from those that cannot. Lactose fermenters, such as Escherichia coli, acidify the medium and produce dark colonies that may have a reflective metallic green sheen; non–lactose fermenters, such as Pseudomonas aeruginosa, produce opaque or translucent colonies (Figure 29.7c).
Figure 29.7 Enriched media.

(a) Burkholderia growing on sheep blood agar (SBA); the red color is from blood suspended in the trypticase soy agar medium. (b) Francisella tularensis growing on chocolate agar; the brown color is due to heat-lysed blood in the trypticase soy agar medium. (c) Escherichia coli, a lactose fermenter (left), and Pseudomonas aeruginosa, a non–lactose fermenter (right) growing on eosin–methylene blue (EMB) agar. The reflective, greenish-yellow sheen of the colonies on the left identifies E. coli as a lactose fermenter.
Blood and Cerebrospinal Fluid Specimens
Pathogens in liquid tissue samples, such as blood and cerebrospinal fluid (CSF), are routinely detected using automated culture systems. For a suspected case of meningitis, a CSF specimen is obtained by a procedure called a lumbar puncture (spinal tap) in which 3–5 ml of fluid is collected drop-by-drop from a needle inserted between lumbar vertebrae. CSF is sterile and clear in a healthy individual, and therefore fluid turbidity and high leukocyte counts are indicators of infection. Similar to other liquid specimens (blood, urine, sputum, wound exudates, etc.), CSF is routinely examined by Gram staining and used to inoculate selective culture media.
The standard procedure for obtaining a blood sample is to aseptically draw 10–20 ml of blood from a vein and inject it into two culture bottles containing general-purpose growth media and an anticoagulant. One bottle is incubated aerobically, while the other is incubated anaerobically (Figure 29.8); both are kept at 35 °C for several days. Automated culture systems (Figure 29.8b) detect growth by measuring turbidity or fluorescence and by periodically monitoring the consumption of O2 or the production of CO2. Most clinically significant bacteria are recovered within 2 days, but growth of some pathogens, including mycobacteria and certain fungi, may take 3 to 5 days or longer. Cultures that exhibit growth are Gram stained and then inoculated onto specialized media for isolation and identification.
Figure 29.8 Growth-dependent diagnostic testing for blood infections.

(a) Cultures to assay both aerobic (left vial) and anaerobic (right vial) bacterial growth are inoculated with an aseptically drawn patient blood sample. (b) After inoculation, both vials in part a are incubated in an automated system that measures growth, for example, by turbidity, production of CO2, or fluorescence. Photos courtesy of Marion General Hospital, Marion, Indiana, USA.
The most common pathogens found in blood include species of Staphylococcus and Enterococcus, but many other bacteria may cause blood infections. Computer databases are used to unambiguously identify clinical isolates by matching their metabolic reactions in various differential media to the biochemical patterns of known pathogens. The biochemical tests incorporated into differential media evaluate the presence or absence of enzymes that catabolize a specific substrate or substrates. Although hundreds of different biochemical tests are known, just a few key tests may be sufficient to identify some pathogens.
Urinary Tract and Fecal Cultures
Urinary tract infections (UTIs) are common, especially in women. In most cases, microorganisms infect the urinary tract by ascending into the bladder from the urethra. UTIs, often introduced through the use of urinary catheters (Figure 29.9), are among the most common healthcare-associated infections. Direct microscopic examination of urine from a UTI patient usually shows the presence of abnormal numbers of bacteria in the urine. A Gram stain may be done directly on urine samples to identify the morphology of urinary tract pathogens, such as gram-negative rods (various enteric bacteria), gram-negative cocci (species of Neisseria), and gram-positive cocci (especially species of Enterococcus).
Figure 29.9 Urinary catheter preparation.

A healthcare professional prepares a urinary catheter. Although the apparatus is pre-sterilized, insertion of the catheter moves microorganisms from the urethra to the bladder and may result in a urinary tract infection, a common HAI.
A significant UTI typically results in bacterial counts of 105 or more cells per milliliter of urine. The most common causative agents of UTIs are enteric bacteria, with E. coli accounting for about 90% of cases. Blood agar is often used for primary enrichment and isolation of urinary tract pathogens. Selective and differential enteric media, such as EMB or MacConkey agar, permit differentiation of gram-negative lactose fermenters from non–lactose fermenters (Figure 29.7c) and inhibit the growth of possible gram-positive contaminants, such as commensal staphylococci. Additional differential and/or selective media may be used to identify urinary tract (or other) pathogens via traditional culturing techniques (**Figure 29.10a,*b***) or rapid and convenient commercial media kits (Figure 29.10c).
Figure 29.10 Growth-dependent diagnostic tests for clinical isolates.

(a) Differential media to assess sugar fermentation. Acid production is indicated by a color change (from red to yellow) of the pH-indicating dye in the medium. The appearance of a bubble in the small, inverted inner tube indicates gas production from fermentation. (b) Diagnostic test for enteric bacteria using triple-sugar iron (TSI) agar. The medium contains glucose, lactose, and sucrose. Organisms able to ferment only glucose cause acid formation only in the bottom of the tube, whereas lactose- or sucrose-fermenting organisms cause acid formation throughout the slant. The breaking up of the agar in the bottom of the tube indicates gas formation. Blackening of the agar is due to the reaction of hydrogen sulfide (from either protein degradation or thiosulfate reduction) with ferrous iron in the medium. From left to right: Fermentation of glucose only (typical of Shigella); growth but no fermentation (typical of Pseudomonas); hydrogen sulfide formation (typical of Salmonella); fermentation of sugars with gas production (typical of Escherichia coli). (c) Miniaturized media kits allow rapid identification of clinical isolates by running many biochemical tests on specimen samples at the same time. Four separate strips, each with a different isolate, are shown.
Proper collection of fecal samples is important for the isolation of intestinal pathogens. Fecal specimens become more acidic during storage, so delay between sampling and processing must be minimized, especially for the isolation of acid-sensitive pathogens, such as Shigella and Salmonella. The fecal sample is placed in a sterile, sealed container for transport to the laboratory. Feces containing blood or pus, as well as feces from patients with suspected foodborne or waterborne infections, are inoculated into suitable media for isolation of potential pathogens. For example, many laboratories use selective and differential media to identify E. coli O157:H7 and Campylobacter species, important intestinal pathogens typically acquired from contaminated food or water (Sections 33.11 and 33.12). Intestinal eukaryotic pathogens, such as Giardia intestinalis (Section 34.4), are identified by direct microscopic observation of parasite cysts in diluted feces or through antigen-detection assays (see Figure 29.19c) rather than by culturing.
Wounds and Abscesses
Infections associated with injuries such as animal bites, burns, or cuts are sampled to recover the relevant pathogen. The results must be interpreted carefully to differentiate between infection and contamination. Wound infections and abscesses often harbor a variety of normal microbiota, and swab samples from such lesions are frequently misleading. For abscesses and other purulent lesions, pus is aspirated with a sterile syringe and needle following disinfection of the skin surface. Internal purulent lesions are sampled by biopsy or from tissues removed in surgery. Gram stains are prepared directly from these specimens and examined microscopically.
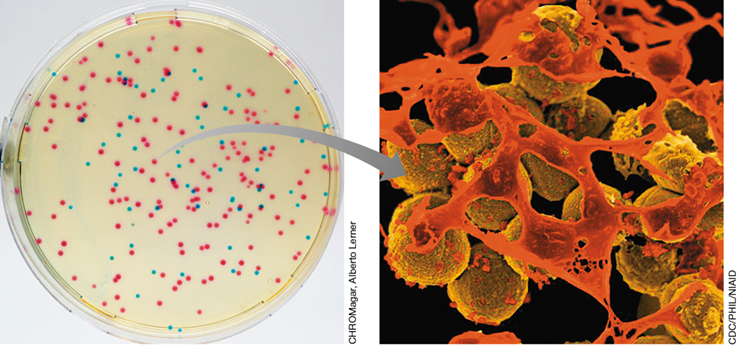
Pathogens commonly associated with wound infections are Staphylococcus aureus, enteric bacteria, P. aeruginosa, and anaerobes, such as species of Bacteroides and Clostridium. Because of the varied oxygen requirements of these bacteria, samples must be obtained, transported, and cultured under anoxic as well as oxic conditions. The major isolation media are blood agar, selective media for enteric bacteria, and enrichment media containing additional supplements and reducing agents for obligate anaerobes. Widely used tools for the detection of MRSA in skin infections are chromogenic agar media. These selective and differential media contain a chromogenic substrate that, when metabolized, causes MRSA to produce distinctly colored colonies (see Explore the Microbial World, “MRSA—A Formidable Clinical Challenge”).
Genital Specimens and Culture for Gonorrhea
Sexually transmitted infections (STIs) that cause a purulent urethral discharge, especially in males, are classified as either nongonococcal or gonococcal urethritis. Nongonococcal urethritis is usually caused by Chlamydia trachomatis (Section 31.13), Ureaplasma urealyticum, or Trichomonas vaginalis (Section 34.4). Gonococcal urethritis is caused by Neisseria gonorrhoeae (Section 31.13).
Cells of N. gonorrhoeae are gram-negative diplococci, a morphology not normally found in microbiota of the urogenital tract. Therefore, a Gram stain of a urethral, vaginal, or cervical smear revealing such cells, often surviving inside neutrophils (Figure 29.6a), is diagnostic for gonorrhea. Chocolate agar, a nonselective enriched medium, is often used for specimens suspected to contain N. gonorrhoeae. A selective medium used for isolation of N. gonorrhoeae is modified Thayer–Martin (MTM) agar (Figure 29.6b). This medium incorporates the antibiotics vancomycin, nystatin, trimethoprim, and colistin to suppress the growth of normal microbiota. These antibiotics have no effect on N. gonorrhoeae or Neisseria meningitidis, a cause of bacterial meningitis (Section 31.5).
Inoculated plates are incubated in a humid atmosphere containing 3–7% CO2 for 24–48 hours and then tested for their oxidase reaction (Figure 29.6b). Oxidase-positive, gram-negative diplococci growing on MTM or chocolate agar are presumed to be gonococci if the inoculum was derived from the urogenital tract. Definitive identification of N. gonorrhoeae requires determination of carbohydrate utilization patterns and immunological or nucleic acid probe tests. Laboratory testing of urogenital samples for N. gonorrhoeae (and the often-associated C. trachomatis) is often done using DNA amplification via polymerase chain reaction (PCR) or other molecular methods.
Culture of Anaerobic Pathogens
The identification of obligately anaerobic bacteria from patient specimens requires special isolation and culture methods (Section 4.16). In general, media for anaerobes do not differ greatly from those used for aerobes, except that they (1) are usually richer in organic constituents, (2) contain reducing agents (usually cysteine or thioglycolate) to remove O2, and (3) contain a redox indicator to show that conditions are anoxic. Collection, handling, and processing of specimens must exclude exposure to air because O2 is toxic to obligate anaerobes. Samples collected by syringe aspiration or biopsy must be immediately transferred to a sealed tube containing O2-free gas, usually with a dilute salt solution containing a reducing agent and a redox indicator to monitor O2 contamination. Specimens are then used to inoculate anoxic media in an automated culture system or in an anoxic “glove box” filled with O2-free gases, usually a mixture of N2 and H2 (Figure 4.29).
Several habitats in the body, including portions of the oral cavity and the lower intestinal tract, are anoxic and support the growth of anaerobic normal microbiota. Other parts of the body may also become anoxic if injury or disease reduces the blood supply to certain tissues, a condition called ischemia. These anoxic sites can then be colonized by obligate anaerobes. Although potentially pathogenic anaerobic bacteria are part of the normal microbiota, their numbers are kept in check through competition with other members of the microbial community. Under certain conditions, however, normally benign anaerobes may become opportunistic pathogens. A key example is Clostridioides (Clostridium) difficile (Table 29.3); this usually harmless member of the normal microbiota of the lower intestinal tract commonly emerges as a healthcare-associated pathogen when extended antibiotic therapy destroys competing microbes (Section 24.11 and Section 30.7).
Check Your Understanding
What are the key requirements for proper collection of clinical specimens, and why is it important that diagnostic tests for these specimens are both highly specific and sensitive?
Identify culture methods and conditions used for blood, wound, urine, fecal, and genital specimens. Of what importance are selective and differential growth media in pathogen detection, and what special conditions must be maintained for the isolation of anaerobic pathogens?
29.4 Choosing the Right Treatment
Pathogens isolated from clinical specimens are identified to confirm medical diagnoses and to guide antimicrobial therapy. Appropriate and effective treatment for many pathogens is based on current experience and practices. For some pathogens, however, decisions about appropriate antimicrobial therapy must be made on a case-by-case basis. Such pathogens include those for which antimicrobial drug resistance is common (for example, gram-negative enteric bacteria), those that cause life-threatening disease (for example, meningitis caused by Neisseria meningitidis), and those that require bactericidal rather than bacteriostatic drugs (Section 4.19) to prevent disease progression and tissue damage. Bactericidal agents are indicated, for example, for bacterial endocarditis (infection of the inner tissues of the heart, such as the heart valves), where total and rapid killing of the pathogen is critical for patient survival.
Minimum Inhibitory Concentration
Antimicrobial susceptibility is measured by determining the smallest amount of agent needed to completely inhibit the growth of the tested organism in vitro (in laboratory culture), a value called the minimum inhibitory concentration (MIC). The traditional way to determine the MIC for a given agent against a given organism is to prepare a series of culture tubes inoculated with the same number of microorganisms. Each tube contains the growth medium with an increasing concentration of the antimicrobial agent. After incubation, the tubes are checked for visible growth (turbidity), and the MIC is the lowest concentration of the agent that completely inhibits the growth of the test organism (Section 4.19 and Figures 4.40 and 4.41).
In modern practice, the MIC of a given antimicrobial agent is typically determined using microliter amounts of media and reagents. For example, a miniaturized version of the MIC test uses a microtiter method with twofold dilutions of several antibiotics in medium inoculated with a standard amount of the test organism (**Figure 29.11*a***). In clinical microbiology laboratories, tests for routine MIC determinations are usually automated using instruments that also allow for species identification of pure cultures obtained from patient specimens (Figure 29.11b, c).
Figure 29.11 Antibiotic susceptibility testing.

(a) Antibiotic susceptibility of a pathogen as determined by the broth dilution method in a microtiter plate. The organism is Pseudomonas aeruginosa. Each row has a different antibiotic in a series of concentrations. The highest concentration of antibiotic is in the well at the left; serial twofold dilutions are made in the wells to the right. In rows 1 and 2, the third well has the lowest concentration of antibiotic that shows no visible growth. In row 3, the antibiotic is ineffective at the concentrations tested because there is growth in all wells. (b, c) An automated system for identifying clinical isolates and determining their antibiotic susceptibility. Card wells (panel c) are inoculated using the attached capillary tube. Following internal incubation, computer-scanned results are available in less than 24 hours. Photos courtesy of Marion General Hospital, Marion, Indiana (USA). (d) For the disk diffusion test, colonies from a pure culture of the pathogen are transferred to a liquid medium and mixed. (e, f) A sterile swab is dipped into the bacterial suspension and streaked evenly over the entire surface of a suitable agar medium. (g) Disks containing known amounts of different antibiotics are placed on the inoculated agar surface. After incubation, zones of inhibition are measured, and antibiotic susceptibility is determined using a standardized chart of zone sizes. For the epsilometer test (Etest®, AB BIODISK, Solna, Sweden), a plastic strip containing an antibiotic gradient (in μg/ml) indicates the MIC at the point where the elliptical zone of inhibition meets the strip. In this example, the MIC for azithromycin (AZ) is 1.0 μg/ml.
Measuring Antimicrobial Susceptibility
The standard assay for antimicrobial activity is the disk diffusion test (Figure 29.11d–g). A Petri plate containing an agar medium is inoculated by evenly spreading a suspension of a pure culture of the suspected pathogen on the agar surface. Known amounts of different antimicrobial agents infused into filter-paper disks are then placed on the surface of the agar. The agents then diffuse from the disks into the agar during incubation, establishing a gradient; the farther the chemicals diffuse away from each disk, the lower is the concentration of the agent. At some distance from each disk, the effective MIC is reached. Beyond this point the microorganism is able to grow, but closer to the disk, growth is absent. A zone of inhibition forms with a diameter proportional to the concentration, solubility, diffusion coefficient, and overall effectiveness of the antimicrobial agent in the disk.
In addition to the disk diffusion test, Figure 29.11g depicts antibiotic susceptibility using the epsilometer test (Etest®). This assay uses a plastic strip infused with a predefined concentration gradient of an antimicrobial agent. When applied to the surface of an inoculated agar plate, the gradient transfers from the strip to the agar and remains stable throughout the incubation period, during which an elliptical zone of inhibition centered along the axis of the strip develops. The concentration of the antimicrobial agent (in μg/ml) is read at the point where the ellipse edge intersects the precalibrated test strip, providing a precise MIC (Figure 29.11g).
Assuming culture conditions are standardized, different antimicrobial agents can be compared to determine which is most effective against the isolated pathogen. The Clinical and Laboratory Standards Institute (www.clsi.org) is responsible for developing, establishing, and constantly updating consensus standards for antimicrobial testing. Hospital infection-control microbiologists produce and examine susceptibility data to generate periodic reports called antibiograms. These reports define the susceptibility of clinically isolated organisms to the antibiotics in current use. Antibiograms are used to monitor control of known pathogens, to track the emergence of new pathogens, and to identify the emergence of antibiotic resistance at the local level.
Check Your Understanding
Describe the disk diffusion test and the Etest for antimicrobial susceptibility. For an individual organism and an antimicrobial agent, what do the results signify?
What is the value of antimicrobial drug susceptibility testing for the microbiologist, the physician, and the patient?
Mastering Microbiology
Art Activity: Figure 29.12 Pattern of infection and immunity in untreated typhoid fever
III: Immunological and Molecular Tools for Disease Diagnosis
III: Immunological and Molecular Tools for Disease Diagnosis
III Immunological and Molecular Tools for Disease Diagnosis
Culture-independent clinical diagnostics, including immunological and molecular-based techniques, are critical for providing rapid and effective healthcare. The quicker an infectious disease is diagnosed, the quicker treatment can begin, and in some cases, prompt treatment is essential to save the patient.
Culture methods for some pathogens, including many viruses and some pathogenic bacteria, are not routinely available, are unreliable, or are prohibitively difficult or expensive to perform. In such cases, growth-independent diagnostic methods are used in clinical, reference, and research laboratories to detect specific pathogens or their products. These include a variety of immunological and molecular assays that can yield a relatively quick and reliable means of identifying individual pathogens or host exposure to pathogens in the absence of cultured organisms.
29.5 Immunoassays and Disease
Many immunoassays use antibodies specific for pathogens or their products for in vitro tests designed to detect specific infectious agents. Patient immune responses, discussed in Chapters 26 and 27, can also be monitored to obtain evidence of pathogen exposure and infection.
Serology and Antibody Titers
The study of antigen–antibody reactions in vitro is called serology. Serological assays detect pathogen-induced antibodies in patient serum and are the basis for a number of diagnostic tests. The specificity of the antibody–antigen reactions associated with serological tests allows one to pinpoint an exposure to a single pathogen, assuming the antigen used to detect antibodies is unique to the pathogen in question. Moreover, serological tests vary considerably in their sensitivity, that is, in the amount of antibody necessary to detect antigen. For example, passive agglutination reactions (see Section 29.6) are fast and easy to perform but require antibody concentrations of up to 6 nanograms (ng, 10−9g) per ml. By contrast, the very sensitive but more technically demanding enzyme immunoassay (EIA) tests require as little as 0.1 ng of antibody per ml and can detect as little as 0.1 ng of antigen (Section 29.7).
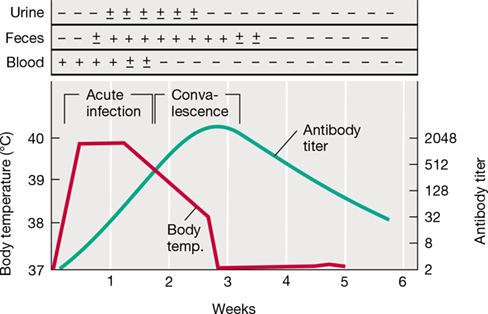
If an individual is infected with a suspected pathogen, the immune response—antibodies to that pathogen—should become elevated. Strong evidence for infection can therefore be obtained by determining the antibody titer directed against antigens produced by the suspected pathogen. The titer is a quantitative measure of antibody level and is defined as the highest dilution (lowest concentration) of serum at which an antigen–antibody reaction is observed (Figure 29.12).
Figure 29.12 Pattern of infection and immunity in untreated typhoid fever patients.

Body temperature indicates acute disease progression over time. Antibody titer is shown as the reciprocal of the highest serial dilution causing agglutination of Salmonella enterica (typhi ) (Section 33.5). The presence of bacteria in blood, feces, and urine was determined from cultures (−, no bacteria; ±, low numbers of bacteria; +, high numbers of bacteria). Bacteria clear from the blood as the antibody titer rises, whereas clearance from feces and urine requires more time. Body temperature drops to normal as the antibody titer rises.
A positive antibody titer indicates previous infection or exposure to a pathogen. For pathogens rarely found in a population, such as the life-threatening hantaviruses (Section 32.2), a single positive test for a pathogen-specific antibody may indicate active infection. In most cases, however, the mere presence of antibody does not indicate active infection. Antibody titers typically remain detectable for long periods after a previous infection has been resolved. To link an acute illness to a particular pathogen, it is essential to show a rise in antibody titer in serum samples taken from a patient during the acute disease and later during the convalescent phase of the disease. Frequently, the antibody titer is low during the acute stage of the infection and rises during convalescence (Figure 29.12). A rise in antibody titer is strong circumstantial evidence that the illness is due to the suspected pathogen.
Skin Tests
A number of pathogens induce a delayed-type hypersensitivity (DTH) response mediated by Th1 cells (Section 28.1). For these pathogens, skin testing may be useful to determine exposure. As an example, a commonly used skin test is the tuberculin test, which consists of an intradermal injection of a soluble extract from cells of Mycobacterium tuberculosis. A positive inflammatory reaction at the site of injection within 48 hours indicates current infection or previous exposure to (or vaccination against) M. tuberculosis (Figure 28.4). Skin tests are routinely used to aid in diagnosis of tuberculosis, Hansen’s disease (leprosy), and some fungal diseases because, as opposed to responses caused by pathogen-specific inflammatory Th1 cells, antibody responses for intracellular and fungal infections are often weak or undetectable.
If a pathogen is extremely localized, there may be little induction of a systemic immune response and no rise in antibody titer or skin test reactivity, even if the pathogen is proliferating profusely at the site of infection. A good example is the infection of urogenital mucosal surfaces with the bacterium Neisseria gonorrhoeae. Gonorrhea does not elicit a systemic or protective immune response, there is no serum antibody titer or skin test reactivity, and reinfection of individuals is common (Section 31.13).
Monoclonal Antibodies
An expanding area of research with broad application in the diagnosis and treatment of disease is the development and use of monoclonal antibodies (mAbs). In contrast to polyclonal antibodies, which occur as a mixture of immunoglobulins produced by many individual B cells and directed at numerous antigenic determinants on a pathogen, mAbs are derived from a B cell clone sensitized to a single antigenic determinant. Thus, an in vitro B cell clone culture produces monospecific mAbs that can be collected for diagnostic or therapeutic purposes. However, antibody-producing B cells are relatively short-lived and normally die within several weeks in cell culture. To produce long-lived B cell clones for commercial mAb production, antibody-producing B cells are fused with myelomas, tumorigenic B cells that divide and grow indefinitely (Figure 29.13). The “immortal” cell lines that result from this fusion are hybrid cells, appropriately called hybridomas. The hybrid cell lines share the biological properties of both fusion partners; they grow indefinitely in vitro and produce antibodies.
Figure 29.13 Production of monoclonal antibodies (mAbs).

The hybridoma can be indefinitely cultured or passed through animals as a tumor. The hybridoma cells are stored as frozen tumor cells that can be thawed and grown in tissue culture or in a suitable animal host.
To produce a particular mAb, a mouse is immunized with the antigen of interest. Antigen-specific B cells then proliferate over several weeks and begin to produce antibodies in the mouse. B cells are then removed from the mouse and mixed with myeloma cells (Figure 29.13), but only a small number of these fuse into antibody-producing hybridomas. The hybridomas are isolated from unfused myeloma cells using a selective HAT medium, so called because it contains the metabolites hypoxanthine (H) and thymidine (T), as well as the cell poison aminopterin (A). The myelomas are unable to grow in this medium because they lack an enzyme that allows them to use the H and T metabolites to circumvent the poisonous effect of aminopterin. Unfused B cells can produce the necessary enzyme, but they die after several days because they cannot divide in culture. Only the fused hybridomas, which combine the properties of both cell types, are able to both produce the necessary enzyme and grow indefinitely.
An enzyme immunoassay (Section 29.7) can be used to identify hybridomas that produce the desired mAb. From a typical fusion, several distinct clones are isolated, each making a different mAb. Once the clones of interest are identified, they can be grown either in the mouse as an antibody-producing tumor or in continuous cell culture. Antibodies can then be harvested from either source.
Commercial production of mAbs has replaced polyclonal antibodies for many immunodiagnostic applications because mAbs are highly specific bioreagents that can be generated with a high degree of reproducibility. Clinical diagnostic tests that use mAbs include immunological typing of bacterial pathogens, identification of cells containing foreign surface antigens (for example, a virus-infected cell), and highly specific blood and tissue typing. Because of their remarkable specificity, mAbs are also used to detect and treat human cancers (Section 28.4). Malignant cells often contain tumor-specific neoantigens on their surfaces (Figure 28.10), and therefore mAbs prepared against these antigens specifically target the cancer cells and can be used to deliver toxins directly to them. As discussed in Chapter 28, mAbs may also be used as checkpoint inhibitors to neutralize immunosuppression within the tumor microenvironment. The use of anticancer mAbs has great potential as an alternative to nonspecific chemical and radiation treatments that damage healthy cells as well as cancer cells.
Check Your Understanding
Explain the reasons for changes in antibody titer for a single infectious agent, from the acute phase through the convalescent phase of the infection.
Describe the method, time frame, and rationale for the tuberculin skin test. What component of the immune response does this test detect?
What advantages do monoclonal antibodies have compared to polyclonal antibodies? How are mAbs produced?
29.6 Precipitation, Agglutination, and Immunofluorescence
29.6 Precipitation, Agglutination, and Immunofluorescence
29.6 Precipitation, Agglutination, and Immunofluorescence
Many clinically useful immunological reactions yield a product visible to the naked eye, such as precipitation or agglutination. Some other reactions are visualized microscopically when fluorescent dyes attached to specific antigens react with their specific antibody. We consider examples of these now.
Precipitation
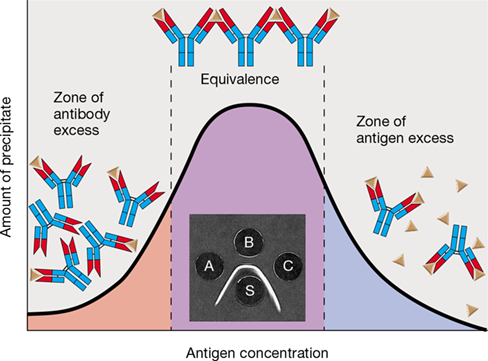
Precipitation results from the interaction of a soluble antibody with a soluble antigen to form an insoluble complex. Tests can be done in liquid test tubes (or capillary tubes) or, as shown in Figure 29.14, in agarose gel. Antigens that have more than one antibody-binding epitope (Section 27.2) can cross-link the bivalent antibodies that recognize them, causing a precipitate to develop from the aggregated antibody–antigen complexes. Precipitation occurs maximally when there are optimal proportions of the two reacting substances. The presence of either excess antigen or excess antibody results in the formation of soluble immune complexes (Figure 29.14).
Figure 29.14 Precipitation reactions between soluble antigen and antibody.

The extent of precipitation is a function of antigen and antibody concentration. Inset photo: Precipitation in agarose gel (immunodiffusion). Well S contains antibodies to cells of Proteus mirabilis. Wells A, B, and C contain soluble extracts of P. mirabilis. An insoluble precipitation band forms where antibody and antigen concentrations are equivalent. Immunoprecipitation photo courtesy of C. Weibull, W.D. Bickel, W.T. Hashius, K.C. Milner, and E. Ribi.
Precipitation reactions carried out in agarose gels, called immunodiffusion tests (Figure 29.14 inset), are especially useful for diagnosing fungal infections, including coccidioidomycosis, histoplasmosis, blastomycosis, and paracoccidioidomycosis (Section 34.2). For these tests, prepared antigen and patient antisera containing antibodies are loaded into separate wells cut into the agarose gel. The reagents diffuse outward from the wells and form precipitation bands where antibody interacts with antigen in optimal proportions (Figure 29.14). Unfortunately, precipitation reactions are not very sensitive; visible precipitation requires microgram quantities of specific antibody rather than the nanogram quantities of more sensitive diagnostic tests. Consequently, with the exception of clinical diagnostic testing for fungal infections, precipitation assays are typically used only in research and reference laboratories.
Agglutination
Agglutination is a reaction between antibody and particle-bound antigen resulting in visible clumping of the particles. Agglutination tests can be done in test tubes, in microtiter plates, or by mixing reagents on glass or coated paper slides. Agglutination tests are quick to perform, inexpensive, highly specific, and reasonably sensitive, making them suitable for large-scale use in clinical applications. Standardized agglutination tests are used for the identification of blood-group antigens (on red blood cells) (**Figure 29.15*a***), as well as pathogens and pathogen products. To determine blood groups, blood samples are mixed with either anti-A antisera or anti-B antisera and the agglutination of red blood cells, called hemagglutination, is assessed (Figure 29.15).
Figure 29.15 Direct agglutination of human red blood cells: ABO blood typing.

(a) A drop of whole blood was mixed with antigen-specific antisera for each reaction. The reaction on the left shows no agglutination with antibody, typical of blood type O. The reaction in the center shows the diffuse agglutination pattern indicative of blood type B. The reaction on the right shows the strong agglutination pattern with large, clumped aggregates typical of blood type A. (b) Table of expected blood typing results for people in the United States.
Agglutination is often assessed using rapid assays that employ small (0.8−μm diameter) latex beads coated with a specific antigen. The beads are mixed with patient serum on a slide and incubated for a short period. If patient antibody binds the antigen on the bead surface, the milky white latex suspension will become visibly clumped, indicating a positive agglutination reaction and exposure to the pathogen.
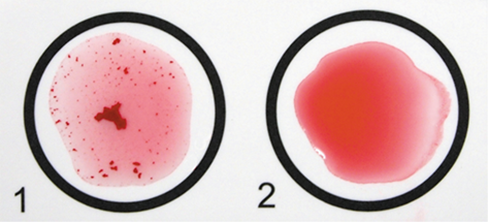
Latex agglutination is also used to detect bacterial surface antigens by mixing cells from a bacterial colony with antibody-coated latex beads. For example, a commercially available suspension of latex beads coated with antibodies to protein A and clumping factor, two proteins found exclusively on the surface of Staphylococcus aureus cells, is specific for identification of clinical isolates of S. aureus (Figure 29.16). Latex bead assays take less than a minute and can be used directly on clinical samples, such as the exudate from a purulent infection, often seen in cases of S. aureus infections. Latex bead agglutination assays have also been developed to identify other common pathogens, such as Streptococcus pyogenes, Neisseria gonorrhoeae, Escherichia coli O157:H7, and the fungus Candida albicans.
Figure 29.16 Latex bead agglutination test for *Staphylococcus aureus*.

In circle 1, a loopful of material from a bacterial colony was mixed in a suspension of microscopic, red latex beads coated with antibodies to two antigens found exclusively on the surface of Staphylococcus aureus cells. The bright red clumps indicate positive agglutination, confirming the colony as S. aureus. Circle 2 is a negative control showing the uniform red color expected in the absence of agglutination.
Immunofluorescence
Antibodies conjugated to fluorescent dyes can be used to detect antigens on intact cells. Such fluorescent antibodies are widely used for diagnostic and research applications. Fluorescent antibody staining methods can be either direct or indirect (Figure 29.17). In the direct method, the antibody that interacts with the surface antigen is itself covalently linked to the fluorescent dye. In the indirect method, the presence of a nonfluorescent primary antibody on the surface of a cell is detected by the use of a fluorescent secondary antibody directed against the nonfluorescent antibody.
Figure 29.17 Fluorescent antibody methods for detection of microbial surface antigens.

Note how indirect immunofluorescence requires a labeled secondary antibody that binds to the primary antibody.
Mastering Microbiology
Art Activity: Figure 29.17 Fluorescent antibody methods for detection of microbial surface antigens
Fluorescent dyes typically conjugated to antibodies include rhodamine B, which fluoresces red-orange, and fluorescein isothiocyanate, which fluoresces yellow-green (Figure 29.18). Once the fluorescent antibodies have bound to cell surface antigens, the complex can be visualized using a fluorescence microscope (Figure 1.25). The cell-bound fluorescent antibodies emit their characteristic fluorescent color when excited with light of particular wavelengths. Fluorescent antibodies can be used for tasks as varied as identifying a microorganism directly in a patient specimen (Figure 29.18) to enumerating T cells in the blood of patients with human immunodeficiency virus/acquired immunodeficiency syndrome (HIV/AIDS).
Figure 29.18 Fluorescent antibody identification of bacteria.

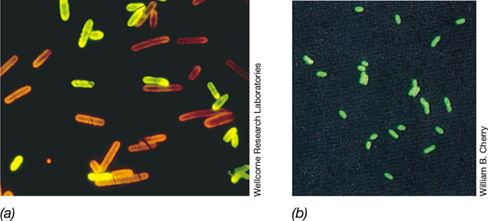
(a) Cells of Clostridium septicum were stained with antibody conjugated with fluorescein isothiocyanate, which fluoresces yellow-green. Cells of Clostridium chauvoei were stained with antibody conjugated with rhodamine B, which fluoresces red-orange. (b) Immunofluorescently stained cells of Legionella pneumophila (legionellosis) from biopsied lung tissue. Individual cells are 2−5μm in length and were stained green with antibodies coupled to fluorescein isothiocyanate.
Mastering Microbiology
Art Activity: Figure 29.20 Enzyme immunoassays (EIAs)
Fluorescent antibodies applied directly to infected host tissues may permit disease diagnosis long before culture methods yield a suspected pathogen (Figure 29.19). For example, a presumptive diagnosis of legionellosis (Legionnaires’ disease), a form of infectious pneumonia (Section 33.4), can be confirmed by staining biopsied lung tissue directly with fluorescent antibodies specific for cell wall antigens of Legionella pneumophila (Figure 29.18b), the causative agent of the disease. Immunofluorescence assays are also used to help diagnose infections from viral pathogens, such as Epstein–Barr virus (EBV) (Figure 29.19a); fungal pathogens, such as Aspergillus (Figure 29.19b); and gastrointestinal parasitic protozoa, such as Giardia intestinalis (Figure 29.19c).
Figure 29.19 Fluorescent antibody identification of pathogens.

(a) Detection of cells infected with Epstein–Barr virus (EBV) using indirect immunofluorescence. The green-stained cells are infected with EBV, which causes mononucleosis and lymphoma. (b) Detection of Aspergillus mold in a case of aspergillosis (Section 34.1 and Table 34.1) using fluorescein-conjugated antibodies. (c) Detection of the waterborne intestinal parasite Giardia intestinalis (Section 34.4) using indirect immunofluorescence.
Check Your Understanding
How is the bivalence of antibodies significant for a precipitation reaction, and under what conditions does precipitation occur maximally?
What are the advantages and disadvantages of agglutination tests versus fluorescent antibody assays? How are the latter used to identify specific cells in complex mixtures, such as blood?
29.7 Enzyme Immunoassays, Rapid Tests, and Immunoblots
29.7 Enzyme Immunoassays, Rapid Tests, and Immunoblots
29.7 Enzyme Immunoassays, Rapid Tests, and Immunoblots
Enzyme immunoassays (EIAs), which include enzyme-linked immunosorbent assays (ELISAs), are immunodiagnostic tools widely used in clinical microbiology and research. EIAs are particularly useful because they are inexpensive, produce no hazardous waste, and are highly specific and sensitive; they can detect as little as 0.1 nanograms of antigen or antibody. Rapid tests are similar to EIAs except that results can often be reported within minutes instead of hours. Many rapid tests provide point-of-care diagnostics but are generally not as specific or sensitive as EIAs.
The comparatively complex and time-consuming immunoblot (Western blot) uses immobilized pathogen proteins as antigens to bind antibodies from patient specimens, providing highly specific evidence for pathogen exposure (see Figure 29.22). Immunoblots are often used to confirm results obtained from other serological tests, including rapid tests and EIAs.
EIAs
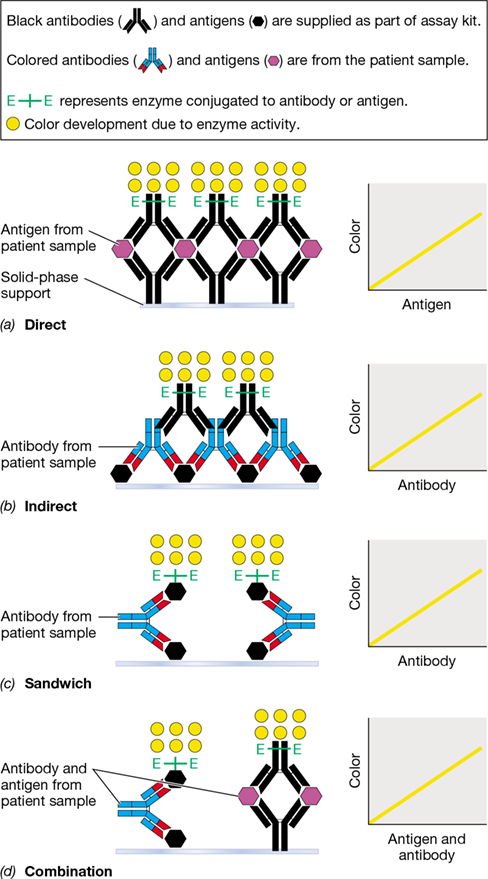
In EIA tests, an enzyme is covalently attached to an antigen or antibody molecule, creating an immunological tool with high specificity and sensitivity. Enzymes typically bound to antigen or antibody include peroxidase, alkaline phosphatase, and β-galactosidase, all of which interact with specific substrates to form colored reaction products that can be detected in low amounts. Four EIA formats are commonly used for evaluation of specimens for infectious disease: direct EIA (detects antigen), indirect EIA (detects antibodies), antigen sandwich EIA (detects antibodies using a sandwich technique), and combination EIA (detects both antigen and antibodies). The principal features of each platform are illustrated in Figure 29.20.
Figure 29.20 Enzyme immunoassays (EIAs).

Patient samples are in color. Assay reagents are shown in black. All assays are fixed to a solid-phase support (light blue). Enzymes bound to antigen or antibody convert substrate to a colored product, shown in yellow. In each assay, the amount of colored product is proportional to the amount of pathogen-specific antibody or antigen derived from a patient sample. (a) The direct EIA uses immobilized pathogen-specific antibody and enzyme-labeled pathogen-specific antibody to detect pathogen antigen in patient samples such as blood. (b) The indirect EIA uses immobilized pathogen antigen and enzyme-labeled antibody directed to immunoglobulin to detect pathogen-specific antibodies in patient samples such as blood. (c) The sandwich EIA uses immobilized pathogen antigen and enzyme-labeled pathogen antigen to detect pathogen-specific antibodies in patient samples such as blood. The sandwich EIA is more sensitive than the direct or indirect EIA methods. (d) The combination EIA uses both the sandwich and direct assays in one platform to identify antibody and antigen in patient samples, maximizing sensitivity. In all cases, it is the enzymatic conversion of a colorless substrate to a colored product, measured spectrophotometrically, that enables quantification of specific antigen and/or antibody.
Direct EIAs are designed to detect antigens, such as virus particles in a blood or fecal sample (Figure 29.20a). Antibodies to a pathogen antigen are coated onto a support, such as a plastic microtiter plate, and the patient sample is then added. After antigen in the sample binds to the antibody, a second antibody, specific to the same antigen and coupled to an enzyme, is added. Finally, enzyme substrate is added, and the enzyme converts the substrate to its colored product in proportion to the amount of patient antigen bound by the enzyme–antibody complex. Direct EIAs are useful for detecting bacterial exotoxins, such as those produced by Vibrio cholerae and Staphylococcus aureus (Section 25.6), as well as a variety of viruses, including those that cause influenza and hepatitis.
Indirect EIAs are used to detect antibodies to pathogens in body fluids (Figure 29.20b). The indirect test starts with pathogen antigen immobilized on a supportive matrix. Patient serum is added, and antibodies (if present) bind to the antigen. Next, an antibody–enzyme complex specific for the patient antibodies is added. Finally, the addition of the enzyme substrate results in the development of a colored product that is proportional to the concentration of patient antibody in the sample. Indirect EIAs are used to detect serum antibodies to a wide variety of bacterial, viral, and eukaryotic pathogens.
The antigen sandwich EIA also detects antibodies to pathogens in body fluids (Figure 29.20c). The sandwich test starts with pathogen antigen immobilized on a support. Patient serum is added, and antibodies (if present) bind to the antigen. Next, the same antigen coupled to enzyme is added, followed by the addition of the enzyme substrate, resulting in the development of colored product that is proportional to the concentration of patient antibody in the sample. This method is especially sensitive because it detects pathogen-specific antibody irrespective of antibody class. This method is often used for HIV screening (the third-generation HIV test) because it can detect IgM produced during the primary immune response to HIV as soon as four weeks after infection. By contrast, most indirect EIAs use anti-IgG as the enzyme-conjugated antibody, delaying observation of antibodies to HIV until the secondary antibody response at least five weeks after infection (Figure 27.10).
The combination EIA, shown in Figure 29.20d, makes use of a direct EIA to detect pathogen antigen and the sandwich method to detect pathogen-specific antibodies, both on a single matrix. This method, used for a fourth-generation HIV test, is more sensitive than the third-generation sandwich test; antigen can be detected as little as 2.5 weeks after HIV infection, reducing the time to treatment.
Rapid Tests
Rapid immunoassay procedures use reagents adsorbed to a fixed support material, such as paper strips or plastic membranes. These point-of-care tests cause a color change on the strip within minutes and serve as rapid diagnostic aids for a variety of infectious diseases, including HIV/AIDS.
For most rapid tests, a body fluid (generally urine, blood, saliva, or sputum) is applied to a sample well in a reagent–support matrix. To detect antigen in patient samples, for example to determine infection by Streptococcus pyogenes (strep throat), the matrix contains soluble antibodies that are specific to the antigen in question and conjugated to a colored molecule called a chromophore (Figure 29.21). As the liquid sample diffuses through the matrix, patient antigens (if present) bind the chromophore-labeled antibodies. Capillary action pulls each labeled antigen–antibody complex through the matrix, where it contacts a single line of fixed antibodies. The labeled antigen–antibody complex binds a fixed antibody and becomes immobilized. As the concentration of labeled complex increases, the chromophore becomes visible as a line of color along the fixed antibody, indicating a positive test for the antigen. Labeled antibodies not bound by antigen concentrate at a second line of fixed antibodies that are specific to the labeled antibody rather than the antigen, thus forming a second colored line that serves as the control.
Figure 29.21 Rapid tests.

(a) A patient specimen containing a mixture of antigens is applied to the sample well of a support matrix. Capillary action pulls the liquid sample through the matrix, and specific antigen (if present) binds soluble, chromophore-labeled antibodies. The labeled antigen–antibody complexes diffuse through the matrix and bind a line of fixed antibodies. A colored line becomes visible as the concentration of labeled complex builds, indicating a positive test for the antigen. Unbound labeled antibodies bind a second line of fixed antibody as a control. (b) From left to right, rapid tests for respiratory syncytial virus (RSV), group A streptococci (GAS), and influenza A/B. The RSV test and the left GAS test show a test line, indicating positive reactions. The right GAS test and the influenza A/B test show only a control line, indicating negative reactions. Photo courtesy of Marion General Hospital, Marion, Indiana (USA).
These tests are valuable for point-of-care analysis and provide rapid diagnostic results that can be reported almost immediately, avoiding the need for delays in patient care or for follow-up visits to obtain test results. The drawback to rapid tests, however, is that they are often less specific or less sensitive than more elaborate assays for the same pathogens. As a result, rapid tests often need to be confirmed by EIA or other tests, such as the immunoblot, discussed next.
Immunoblots
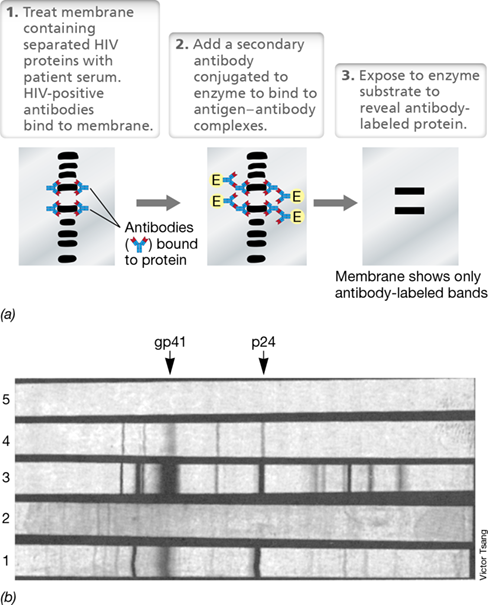
Immunoblot methodology requires the separation of proteins on a polyacrylamide gel, the transfer (blotting) of the proteins from the gel to a nitrocellulose or nylon membrane, and finally, the identification of the proteins using specific antibodies (**Figure 29.22*a***). The HIV immunoblot (Figure 29.22b) can be used to accurately diagnose HIV infection, but although it is highly specific, it is generally not used as a screening tool because it is less sensitive, more time consuming, and more expensive than the HIV EIA. However, because the HIV EIA occasionally yields false-positive results, the immunoblot method is often used to confirm positive EIA tests. The HIV immunoblot procedure is similar to immunoblot methods used to diagnose infection by other pathogens. In general, immunoblots are used to detect pathogen-specific antibody in patient samples.
Figure 29.22 The immunoblot (Western blot) and its use in the diagnosis of human immunodeficiency virus (HIV) infection.

(a) Protocol for an immunoblot. (b) The molecules p24 (capsid protein) and gp41 (envelope glycoprotein) are diagnostic for HIV. Lane 1, positive control serum (from known AIDS patients); lane 2, negative control serum (from healthy volunteer); lane 3, strong positive from patient sample; lane 4, weak positive from patient sample; lane 5, reagent blank to check for background binding.
To perform the HIV immunoblot, membrane strips containing fixed HIV proteins are incubated with the patient serum sample. If the sample is HIV-positive, patient antibodies will bind to the HIV proteins on the membrane. To detect whether antibodies from the serum sample have bound to HIV antigens, a detecting antibody, anti–human IgG conjugated to an enzyme, is added to the strips. If the detecting antibody binds, the activity of the conjugated enzyme, after addition of substrate, will form a colored band on the strip at the site of antibody binding. The patient is HIV-positive if the positions of the bands in the patient sample match those of a positive control; a negative control serum is also analyzed and must show no bands (Figure 29.22b). As the test is mostly used to confirm positive EIA results for HIV (or correct false positives), variations in band intensity do not affect interpretation of the results.
Check Your Understanding
Compare direct, indirect, sandwich, and combination EIAs with respect to their ability to identify infection with a particular pathogen.
Compare the advantages and disadvantages of EIA, rapid tests, and immunoblots with respect to speed, sensitivity, and specificity.
29.8 Nucleic Acid–Based Clinical Assays
In Section 12.1 we discussed how the polymerase chain reaction (PCR) amplifies nucleic acids, forming multiple copies of target sequences. PCR techniques can employ primers for a pathogen-specific gene to examine DNA derived from suspected infected tissue, even in the absence of an observable or culturable pathogen. As a result, PCR-based tests are widely used in the clinical lab for pathogen identification, and they are particularly useful for identifying viruses and other intracellular pathogens that are difficult or impossible to culture using current techniques. PCR methods are extremely sensitive and do not depend on pathogen isolation or growth, and no detection of an immune response to the pathogen is required. Instead, microbe-specific nucleic acid sequences are detected in the assays.
Nucleic Acid Hybridization and Amplification
Nucleic acid hybridization (Section 12.1) is the central theme of nucleic acid–based molecular methods. In clinical medicine, hybridization methods are employed to identify specific pathogens in patient samples by using unique nucleic acid probes to detect the presence of specific DNA sequences. Nucleic acid probes are single-stranded DNA molecules having a sequence complementary to that of a gene of interest. A DNA probe oligonucleotide may be less than 100 base pairs or up to several kilobases in length. If a microbe from a clinical specimen contains DNA or RNA sequences complementary to the probe, the probe will hybridize (following appropriate sample preparation to yield single-stranded target molecules), forming a double-stranded molecule (Figure 29.23). To detect the hybridization reaction, the probe is labeled with a reporter molecule, which is usually a fluorescent compound, but radioisotopes or enzymes may also be used.
Figure 29.23 Nucleic acid probe methodology in clinical diagnostics.

(a) Membrane filter assay. The reporter can be a radioisotope, a fluorescent dye, or an enzyme. (b) Dipstick assay. Dual reporter and capture probes are used. The capture probe contains a poly(A) tail that hybridizes to a poly(T) oligonucleotide affixed to the dipstick. Binding of the target DNA–reporter complex is usually detected as a visible color change.
To carry out a probe assay, samples are treated with strong alkali, usually sodium hydroxide (NaOH), to lyse the cells and partially denature the pathogen DNA, forming single-stranded DNA molecules (Figure 29.23). Incubation at an appropriate temperature facilitates formation of a stable duplex between target DNA and probe DNA. The extent of hybridization is measured using the reporter molecule attached to the probe. Some assays use two-component probes that function as both a reporter probe and a capture probe; the addition of a sequence tag allows the hybridized molecule to be affixed to a matrix, usually a dipstick, for detection purposes (Figure 29.23b).
Nucleic acid hybridization also plays a critical role in the various PCR-based techniques used to amplify target DNA or RNA molecules. PCR analysis begins with the extraction of DNA or RNA from the sample to be tested. Next, the nucleic acid must be amplified using appropriate gene-specific nucleic acid primers. These short oligonucleotides (typically 15–27 base pairs in length) are not used as probes but instead function to jump-start DNA polymerase during PCR amplification of pathogen-specific genes. Lastly, the amplified nucleic acid product (the amplicon) is visualized, a procedure that may involve gel electrophoresis or, more often in clinical laboratories, fluorescence. The presence of the appropriate amplified gene segment confirms the presence of the pathogen.
Quantitative PCR and Reverse Transcription PCR
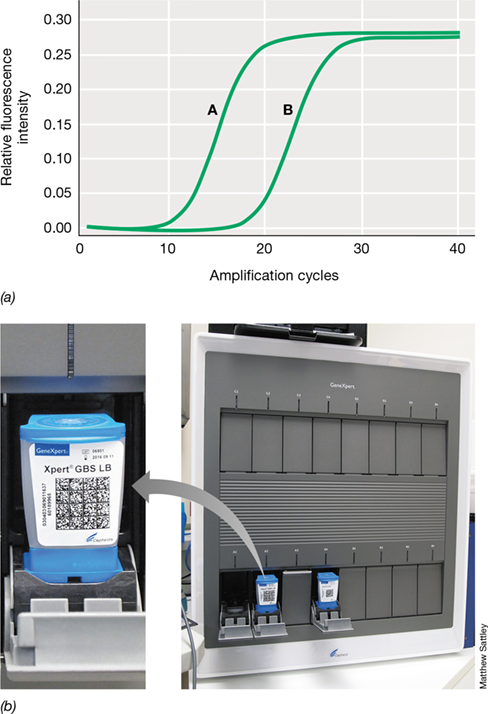
Many clinical PCR tests employ quantitative real-time PCR (qPCR). This process uses fluorescent probes to label PCR amplicons, thereby allowing the accumulation of target DNA to be visualized. Because probe fluorescence increases upon binding to DNA, the level of fluorescence increases proportionally as the target DNA is amplified. The fluorescent probes may be either nonspecific or specific for the target DNA. For example, the dye SYBR Green binds nonspecifically to double-stranded DNA and fluoresces only when bound. When added to the PCR mixture, SYBR Green fluorescence indicates the presence of double-stranded DNA produced by the amplification process (**Figure 29.24*a***). By contrast, gene-specific fluorescent probes, made by attaching a fluorescent dye to a short DNA probe specific to a target sequence, fluoresce only when double-stranded DNA of the correct sequence accumulates.
Figure 29.24 Quantitative real-time polymerase chain reaction (qPCR) for clinical diagnostics.

(a) DNA extracted from a gram-negative bacterial culture was monitored for expression of 16S rRNA (curve A) and npt (curve B), a kanamycin resistance marker, using gene-specific primers. The fluorescent dye SYBR Green was added to the PCR mixture and used to visualize amplified DNA as it formed. The curve on the left (A) had 0.15 fluorescence units after 15 cycles, while the curve on the right (B) had 0.15 fluorescence units after 22 cycles, indicating that the 16S rRNA had a higher abundance of template DNA than npt in this strain. (b) qPCR instrumentation in a clinical laboratory. The single-use cartridges contain all necessary components for the qPCR reaction, including group-specific primers and fluorescent dyes, and pathogens can be identified in less than 2 hours. The cartridge on the left is specific for detection of group B streptococci (Streptococcus agalactiae). Photos courtesy of Marion General Hospital, Marion, Indiana (USA).
Because qPCR amplification can be monitored continuously via fluorescence, visualization by gel electrophoresis is not necessary to confirm amplification. Using modern instrumentation, such as that shown in Figure 29.24b, detection of a gene diagnostic for a particular pathogen in a clinical sample may be performed in about 2 hours. Moreover, by monitoring the rate of fluorescence increase in the PCR reaction, it is possible to accurately determine the amount of target DNA present in the original sample (Figure 29.24a). Thus, qPCR can be used to assess the abundance of a pathogen in a sample by quantifying a gene characteristic for that particular organism.
Another variation of basic PCR is reverse transcription PCR (RT-PCR), which uses pathogen-specific RNA to produce complementary DNA (cDNA) directly from patient samples (Section 12.1). This technology is especially useful for the detection of RNA viruses, including retroviruses such as HIV. The first step in RT-PCR is to use the enzyme reverse transcriptase to make a cDNA copy of an RNA sample. PCR is then used to amplify the cDNA. By isolating RNA in a sample and making cDNA copies of the corresponding gene(s), one can employ qPCR to monitor the expression of a particular gene from a pathogen. The amplified DNA can then be sequenced or probed for identification.
Qualitative PCR
Some diagnostic tests based on the qPCR format use a slightly different amplification protocol and an additional step to identify pathogen-associated genes. This method, called qualitative PCR, uses labeled hybridization primers that are incorporated into an amplicon product of a qPCR reaction.
In the example shown in Figure 29.25, the hybridization probes are targeted to the DNA pol gene of herpes simplex 1 and 2 viruses (HSV-1 and HSV-2)(Section 11.7). The amplicon is detected using two distinct hybridization probes labeled with fluorescent dyes. The probes hybridize to an internal sequence of the amplified fragment during the annealing phase of the PCR cycle. After hybridization to the template DNA, the probes are excited by a light source in the PCR instrument. The emitted fluorescence is then measured, and, after the PCR cycle, a melting curve analysis is performed to differentiate between samples positive for HSV-1 and HSV-2. Because of nucleotide polymorphisms between the DNA pol genes of the two virus subtypes, the melting curve for HSV-1 is distinct from that of HSV-2 (Figure 29.25). The results are compared to internal assay control reactions, and an unambiguous diagnosis of viral infection can be obtained within hours.
Figure 29.25 Qualitative PCR for the *pol* gene of HSV-1 (herpes simplex 1 virus) and HSV-2.

DNA from a patient sample was assayed for the pol gene of both HSV-1 and HSV-2 following quantitative PCR (qPCR). Two fluorescent-labeled probes hybridize with an internal sequence of the amplified fragment of each viral genome during the PCR cycle. After hybridization to the template DNA, the probes are excited by a light source, and their fluorescence is measured. After the PCR cycle, each virus shows a distinct DNA melting curve. The melting profile in the patient sample (red) corresponds to the HSV-2 standard (green), indicating infection with HSV-2.
With a solid foundation of clinical diagnostics in hand, we move on in Chapter 30 to explore how infectious diseases are transmitted, tracked, and controlled in the fast-moving field of epidemiology.
Check Your Understanding
What advantage(s) does nucleic acid amplification have over standard culture methods for identification of microorganisms? What are the disadvantages?
How do quantitative PCR (qPCR) and qualitative PCR differ?
Explore the Microbial World MRSA—A Formidable Clinical Challenge
Explore the Microbial World MRSA—A Formidable Clinical Challenge
MRSA—A Formidable Clinical Challenge
Staphylococcus aureus is an opportunistic human pathogen that colonizes an estimated one-third of the population. In such individuals, this gram-positive bacterium usually exists as an innocuous member of the normal microbiota of the skin and mucous membranes, especially in the nasal epithelium. Although most complications from staphylococci occur in the form of local skin infections, S. aureus may in some cases invade other tissues of the body, including the bloodstream, where a host of virulence factors it produces may transform this bacterium from a harmless commensal to a serious pathogen capable of causing life-threatening disease.
Virulence factors of S. aureus include coagulase and clumping factor, two proteins that precipitate blood plasma components and promote the formation of a protective matrix around the bacterial cells that inhibits the activity of phagocytes at sites of infection. In addition, protein A is a surface protein on S. aureus that obstructs opsonization by antibodies and complement (Section 26.9), effectively camouflaging the pathogen and further impeding phagocytosis. S. aureus also produces several potent exotoxins, including α -hemolysin (lyses blood cells), enterotoxin B (causes food poisoning), and toxic shock syndrome toxin-1 (causes life-threatening toxic shock).
Many S. aureus infections are effectively treated using β -lactam antibiotics, such as various penicillins, but the number of strains resistant to these drugs is increasing as global use of antibiotics remains extremely high (see Figure 28.13a). Infections caused by multidrug-resistant strains of S. aureus are often treated with methicillin, a powerful semisynthetic β -lactam drug that is among the last treatment options available in these cases. However, an alarming percentage of S. aureus strains have also developed resistance to methicillin in recent years. These methicillin-resistant S. aureus (MRSA) strains have been especially prevalent as healthcare-associated infections (Section 29.2).
Clinical diagnosis of MRSA infections depends upon either culture-based techniques, which often include the use of chromogenic agar media (Figure 1) or nucleic acid–based tests (Section 29.8). Confirmation of infection must be followed by antibiotic susceptibility testing (Section 29.4) to determine the best treatment strategy. Typically, treatments are case-specific and require a non-β -lactam antibiotic such as vancomycin, tetracycline, or sulfa drugs (Section 28.5), often administered intravenously.
Figure 1 Methicillin-resistant *Staphylococcus aureus* (MRSA).

Colonies of MRSA on this chromogenic agar medium (left) appear pink, whereas colonies of other bacteria appear blue. The colorized scanning electron micrograph on the right shows cells of MRSA (yellow) embedded in a matrix of cellular debris (orange).
The global incidence of MRSA infection remains high; almost 80,000 cases are documented every year in the United States alone, and several regions of the world have reported increases in MRSA prevalence in recent years, especially in India. Interestingly, the prevalence of healthcare-associated MRSA infections has steadily declined in recent years while that of community-associated MRSA infections has increased. The United States Centers for Disease Control and Prevention estimates that MRSA carriers comprise 2% of the population. Considering its prevalence and extensive multidrug resistance, MRSA may continue to prove a difficult pathogen to control.
Chapter Review
Go to Mastering Microbiology for videos, animations, practice tests, and more.
I Microbiology and the Healthcare Environment
29.1 Clinical laboratory safety requires training and planning to prevent contamination and possible infection of laboratory workers. Specific precautions and procedures proportional to the risk of infection by a given agent, designated by biosafety levels (BSL), must be in place to handle contaminated materials and patient specimens.
Q How are most laboratory-associated infections contracted? What action can be taken to prevent laboratory infections?
29.2 Patients in healthcare facilities are unusually susceptible to infectious disease because of their compromised health and potential exposure to various pathogens in the facilities. Many healthcare-associated infections are caused by drug-resistant pathogens.
Q Healthcare environments are conducive to the spread of infectious diseases. What are some of the reasons that infections can spread so easily in the clinical setting?
II Isolating and Characterizing Infectious Microorganisms
29.3 Appropriate sampling, observation, and culture techniques are necessary to isolate and identify potential pathogens. The selection of techniques requires knowledge of the ecology, physiology, and metabolism of suspected pathogens. Most pathogens exhibit unique metabolic patterns when grown on specialized selective and differential media. Growth-dependent patterns provide information helpful for unambiguous pathogen identification.
Q Why is it important to process clinical specimens as rapidly as possible? What special procedures and precautions are necessary for the isolation and culture of anaerobes?
29.4 Pathogens isolated from clinical samples are often tested for antibiotic susceptibility to ensure appropriate antibiotic therapy. Testing is based on the minimum inhibitory concentration of an agent necessary to completely inhibit growth of a pathogen.
Q Describe the disk diffusion test for antibiotic susceptibility. Why should potential pathogens isolated from patient samples be tested for antibiotic susceptibility?
III Immunological and Molecular Tools for Disease Diagnosis
29.5 An immune response is a natural outcome of infection. Specific immune responses characterized by a rise in antibody titers and positive T cell–mediated skin tests can be used to provide evidence of infections and to monitor convalescence. Monoclonal antibodies reproducibly provide specificity for a wide range of diagnostic and therapeutic purposes.
Q Why does antibody titer rise after infection? Is a high antibody titer indicative of an ongoing infection? Explain. Why is it necessary to obtain an acute and a convalescent blood sample to monitor infections?
29.6 Precipitation and agglutination reactions produce visible results involving antigen–antibody interactions. Fluorescent antibodies are used for quick, accurate identification of pathogens and other antigenic substances in tissue samples, blood, and other complex mixtures. Fluorescent antibody–based methods can be used for identification of a variety of microbial cell types.
Q Why are agglutination tests so widely used in clinical diagnostics? How are fluorescent antibodies used to diagnose diseases? What advantages do immunofluorescent techniques have over traditional culturing?
29.7 Enzyme immunoassays (EIAs), rapid tests, and immunoblots are sensitive and specific immunological assays. These tests can be engineered to detect either antibody or antigen for diagnosis of infections by any of a large number of pathogens.
Q EIAs are extremely sensitive diagnostic tools. Why, then, is the immunoblot (Western blot) procedure used to confirm screening tests that are positive for human immunodeficiency virus (HIV)?
29.8 Nucleic acid amplification (PCR) methods are applied as extremely specific diagnostic tools used for a large number of pathogens. Quantitative PCR (qPCR) and qualitative PCR techniques provide quantification and identification of pathogens, and reverse transcription PCR (RT-PCR) is especially useful for detecting RNA viruses.
Q Distinguish between quantitative and qualitative PCR. How does qualitative PCR expand upon the qPCR technique?
Application Questions
Define the procedures you would use to isolate and identify a new pathogen. Keep in mind Koch’s postulates (Figure 1.33) as you form your answer. Be sure to include growth-dependent assays, immunoassays, and molecular assays. Which of your assays could be adapted to be used as a routine test for rapid clinical diagnosis?
Imagine yourself as a clinical microbiologist with all of the diagnostic tools described in this chapter available for your analyses. Which tool(s) would you use (and why) for the following cases? (1) A patient has a life-threatening infection caused by a difficult-to-culture bacterium, and treatment of the infection is absolutely dependent on an extremely rapid identification of the pathogen. (2) A patient has a less severe bacterial infection with a pathogen that is easily culturable and treatable.
Chapter Glossary
a reaction between antibody and particle-bound antigen resulting in visible clumping of the particles Differential media
growth media that allow identification of microorganisms based on phenotypic properties Enzyme immunoassay (EIA)
a test that uses antibodies or antigens linked to enzymes to detect antigens or antibodies in body fluids Fluorescent antibody
an antibody molecule covalently modified with a fluorescent dye that makes the antibody visible under fluorescent light Healthcare-associated infection (HAI)
an infection acquired by a patient in a healthcare facility, particularly during a stay in the facility. Also called a nosocomial infection. Immunoblot (Western blot)
the use of labeled antibodies to detect specific proteins after separation by electrophoresis and transfer to a membrane Minimum inhibitory concentration (MIC)
the smallest amount of an antimicrobial substance that prevents growth of the target microorganism Monoclonal antibody (mAb)
a single type of antibody made by a single B cell hybridoma clone Point-of-care diagnostics
clinical testing that produces a clear medical result and a treatment plan within the same clinical visit Precipitation
a reaction between antibody and a soluble antigen resulting in a visible, insoluble complex Selective media
culture media that allow the growth of certain organisms while inhibiting the growth of others through one or more added media components Sensitivity
the lowest amount of antigen that can be detected by a diagnostic test Serology
the study of antigen–antibody reactions in vitro Specificity
the ability of a diagnostic test to identify a specific pathogen Titer
the number of individual particles of a substance, such as antibodies or infectious virions, per unit volume of a solution